2024: Volume 4, Issue 4
Past Issues
 Abstract
Abstract  PDF
PDFCutaneous Metastases as Indicators of Advanced Renal Cell Carcinoma: A Case Report
Diana Alejandra Vázquez Medrano1,*, Ma. Teresa de Jesús Vega González2, Isaac Maya González3, Ma. Delia Perez Montiel Gomez4, Dorian Yarih Garcia-Ortega5
1Dermatology Fellow, Hospital General Tacuba, ISSSTE, Lago Ontario 36, Tacuba, Miguel Hidalgo, 11410 Mexico City, CDMX, Mexico
2Dermatologist, National Cancer Institute (Instituto Nacional de Cancerología), Mexico City, Mexico
3Medical Student Instituto Politécnico Nacional Centro disciplinario de las Ciencias de la Salud, Mexico
4Oncological Pathology, National Cancer Institute (Instituto Nacional de Cancerología), Mexico City, Mexico
5Surgical Oncologist, Department of Skin, Soft Tissue, and Bone Tumors, National Cancer Institute (Instituto Nacional de Cancerología), Mexico City, Mexico
*Corresponding author: Diana Alejandra Vázquez Medrano, Dermatology Fellow, Hospital General Tacuba, ISSSTE, Lago Ontario 36, Tacuba, Miguel Hidalgo, 11410 Mexico City, CDMX, Mexico; Phone: 5580401639; Email: [email protected]
Received Date: October 27, 2024
Publication Date: December 06, 2024
Citation: Vázquez Medrano DA, et al. (2024). Cutaneous Metastases as Indicators of Advanced Renal Cell Carcinoma: A Case Report. Dermis. 4(4):25.
Copyright: Vázquez Medrano DA, et al. © (2024).
ABSTRACT
Background: Cutaneous metastases from renal cell carcinoma (RCC) are rare occurrences that often signify advanced disease and poor prognosis. Dermatological presentations can vary widely, making diagnosis challenging but crucial for timely management. Case Reports: We present two cases highlighting the dermatological manifestations of cutaneous metastases from RCC. The first case involves a 56-year-old male with advanced RCC and lung metastasis, who developed a nodular neoplasm on the first finger of his right hand, confirmed as RCC metastasis. The second case describes a 57-year-old male diagnosed with a malignant kidney tumor that metastasized to the scalp. Dermoscopy revealed a papule with reddish-violet, vascular-appearing areas featuring amorphous milky pink-to-red structures and scattered telangiectasias. Conclusions: Cutaneous metastases, although uncommon, can be the first sign of RCC progression or recurrence. Dermatologists should consider metastatic RCC in the differential diagnosis of new skin lesions, especially in patients with a history of RCC.
Keywords: Renal Cell Carcinoma, Cutaneous Metastasis, Dermatology, Skin Lesions, Dermoscopy, Case Report
INTRODUCTION
Renal cell carcinoma accounts for approximately 3% of all adult malignancies and is notorious for its potential to metastasize to unusual sites, including the skin [1,2]. Cutaneous metastases occur in about 3.3% of RCC cases and are often a marker of advanced disease with a poor prognosis [3]. These metastases typically present as rapidly growing, painless nodules that may be mistaken for benign skin conditions [4]. Early recognition and diagnosis are essential for timely management and can significantly impact the patient's quality of life.
Renal cell carcinoma is a complex malignancy that represents about 3% of all adult cancers and is notable for its ability to metastasize to unusual sites, including the skin. [1,2]. This observation applies to renal cancer, regardless of its subtype. Approximately 65% of patients with RCC present with localized tumors, while 35% develop metastases or experience recurrences, which necessitates systemic therapy [1,5]. Treatment options include kinase inhibitors and immune checkpoint inhibitors, which have transformed both therapy and prognosis. The most common metastatic sites for RCC, in descending order, include the lungs, bones, central nervous system, liver, adrenal glands, and skin.
Cutaneous metastases from RCC typically present as nodular lesions, ranging from reddish to purplish in color, and often appear between 6 months to 5 years after diagnosis [2]. It has been suggested that metastatic spread may occur through lymphohematogenous dissemination, direct extension, or even through iatrogenic implantation [1].
METHODS
Patient Selection and Consent
Patients included in this study were selected based on their history of renal cell carcinoma (RCC) and the clinical suspicion of cutaneous metastases.
Diagnostic Procedures
The diagnostic process involved a comprehensive approach combining clinical, dermoscopic, histological, and immunohistochemical evaluations:
- Clinical and Dermoscopic Assessment: Both lesions were examined using a dermoscope model: 3Gen DermLite DL200 with polarized light. The dermoscopic evaluation of the lesion in case 2 revealed vascular-appearing areas with amorphous milky pink-to-red structures and scattered telangiectasias. In contrast, the lesion in case 1 was more advanced, presenting with a hemorrhagic crust that obscured dermoscopic details, and was therefore not included in the study.
- Biopsy Technique: Lesions were biopsied using a punch and incisional method to obtain representative tissue samples.
- Histology and Staining Methods: Tissue sections were stained with hematoxylin and eosin (H&E) for initial histopathological evaluation. Immunohistochemical staining was conducted using markers such as CD10, vimentin, and PAX8 to confirm the diagnosis of metastatic RCC and differentiate it from other neoplasms.
CASE PRESENTATION
CASE 1
A 56-year-old male with a known history of advanced RCC with lung metastasis presented to the dermatology clinic with a rapidly growing nodule on the first finger of his right hand. The lesion appeared two weeks before presentation and measured approximately 1 cm in diameter (Figure 1a). It was firm, non-tender, and reddish in hue.
We performed an excisional biopsy, and histopathological examination revealed clusters of clear cells with prominent nucleoli, consistent with metastatic clear cell RCC. Immunohistochemical staining was positive for CD10, vimentin and PAX 8 confirming the diagnosis [6,7].
Two weeks post-biopsy, the lesion site showed signs of healing without complications (Figure 1b). We referred the patient back to oncology for further management. Given the progression of metastatic disease, we initiated systemic therapy with a tyrosine kinase inhibitor.
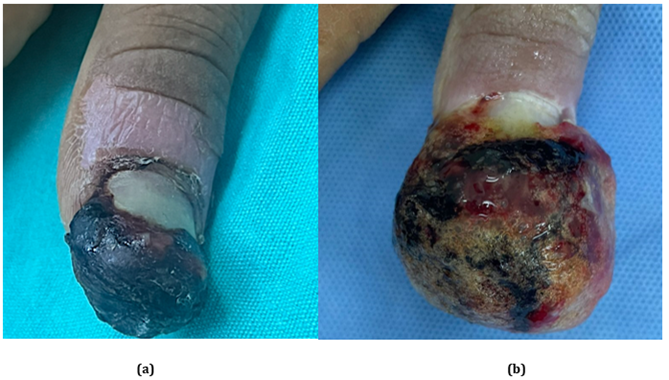
Figure 1a. 56-year-old male diagnosed with advanced renal cancer with lung metastasis, presenting a nodular neoplasm on the first finger of the right hand, consistent with renal metastasis. Figure 1b. Two weeks post-biopsy.
CASE 2
A 57-year-old male, previously diagnosed with a malignant kidney tumor, presented with a solitary papule on his scalp. He noticed the lesion three weeks earlier, gradually increasing in size. (Figure 2a). Dermoscopic examination revealed a papule with reddish-violet, vascular-appearing areas featuring amorphous milky pink-to-red structures with multiple shades and scattered telangiectasias (Figure 2b). A punch biopsy and histopathology showed nests of clear cells typical of RCC metastasis. Immunohistochemical studies were positive for PAX 8, CD10 and vimentin and negative for cytokeratin 7 (CK7), confirming the diagnosis. Skin sample shows positive expression for PAX8 (Figure 2c) [6,7].
Further imaging studies revealed additional metastases to the lungs and bones. We started the patient on immunotherapy with an immune checkpoint inhibitor.
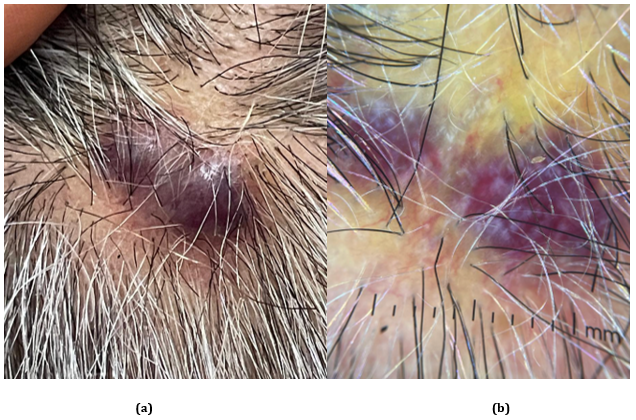
Figure 2a. A 57-year-old male diagnosed with a malignant kidney tumor with metastasis to the scalp. Figure 2b. Dermoscopy reveals a papule with reddish-violet, vascular-appearing areas, featuring amorphous milky pink-to-red structures with multiple shades and scattered telangiectasias.
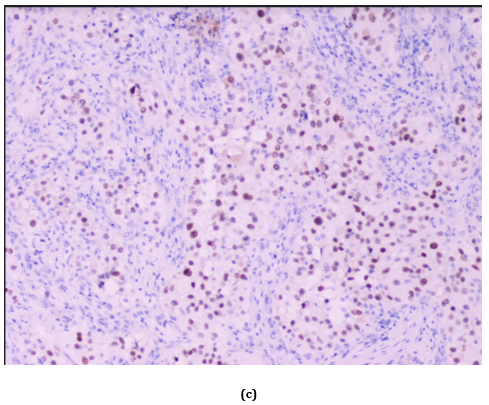
Figure 2c. Positive expression of PAX8 in the skin biopsy sample.
DISCUSSION
Cutaneous metastases from renal cell carcinoma (RCC) are rare but significant indicators of advanced disease progression [3,8]. Their occurrence often signifies widespread metastatic involvement and is associated with a poor prognosis, emphasizing the critical need for early detection and intervention, especially considering that the most common metastatic sites in renal cell carcinoma, in descending order, are the lungs, bones, central nervous system, liver, adrenal glands, and skin [1-3].
The two cases presented highlight the diverse dermatological manifestations of RCC metastases and underscore the importance of considering metastatic disease in the differential diagnosis of new skin lesions, particularly in patients with a known history of RCC.
In the first case, a 56-year-old male with advanced RCC and lung metastasis developed a nodular neoplasm on the first finger of his right hand. Acral metastases involving the distal extremities, such as fingers and toes, are uncommon and account for a small fraction of cutaneous metastases [9]. These lesions are often misdiagnosed due to their rarity and nonspecific clinical presentation, frequently mistaken for benign conditions like pyogenic granulomas, warts, or infectious processes. The rapid onset and growth of the lesion in this patient, coupled with its unusual location, should prompt clinicians to consider metastatic disease in the differential diagnosis. Histopathological examination remains indispensable for accurate diagnosis, as it can reveal the characteristic clear cell morphology of RCC metastases. Biopsy shows clear cells exhibiting nuclear atypia or nuclear predominance in a hexagonal pattern reminiscent of a honeycomb structure. The most frequently reported immunohistochemical markers are vimentin and CD10. A retrospective observational study conducted by Sutthiporn Namnak et al. determined that CD10 was the most prominently expressed marker in clear cell, papillary, and chromophobe RCC. The study recommended that the initial immunohistochemical panel for diagnostic evaluation include vimentin, CD10, and CK7 [9].
The second case involves a 57-year-old male who presented with a scalp lesion that dermoscopically exhibited reddish-violet areas with amorphous milky pink-to-red structures and scattered telangiectasias. The scalp is a relatively common site for cutaneous metastases due to its rich vascular supply and proximity to systemic circulation [2,10]. Dermoscopic features of RCC cutaneous metastases often reflect their vascular nature, presenting with polymorphous vascular patterns, including linear irregular vessels, dotted vessels, and milky-red areas [11]. These features indicate neoplastic angiogenesis driven by overexpression of vascular endothelial growth factor (VEGF), a hallmark of RCC pathogenesis [5]. Recognizing these dermoscopic patterns is crucial for dermatologists, as it aids in differentiating malignant lesions from benign vascular tumors.
The pathogenesis of RCC cutaneous metastases involves hematogenous dissemination facilitated by the tumor's intrinsic angiogenic properties. Mutations or loss of function in the von Hippel-Lindau (VHL) gene leads to the upregulation of hypoxia-inducible factors and subsequent overproduction of VEGF, promoting angiogenesis and tumor proliferation as in renal cell carcinoma patients [12]. This process contributes to primary tumor growth and enhances the potential for metastatic spread to distant sites, including the skin. The skin's rich vascular and lymphatic networks provide a favorable environment for tumor cell implantation and growth [13]. Additionally, the tendency for RCC to invade venous structures can facilitate the hematogenous spread of tumor cells [14].
Clinically, cutaneous metastases from RCC can present a diagnostic challenge due to their variable appearance. Lesions are often asymptomatic, rapidly growing nodules or papules on the skin that may ulcerate or bleed. Their color can range from skin-colored to reddish or purplish hues, reflecting the underlying vascularity [4,15]. In some cases, they may mimic benign dermatological conditions such as cysts, hemangiomas, or infectious processes, leading to misdiagnosis or delayed diagnosis. Therefore, a high index of suspicion is necessary, particularly in patients with a history of RCC.
Histopathological evaluation is critical for definitive diagnosis. Skin biopsy in metastatic RCC typically shows nests or sheets of clear cells with abundant clear cytoplasm due to glycogen, lipid content, and prominent nucleoli [16]. The architectural pattern may be solid, alveolar, or tubular. Immunohistochemical staining enhances diagnostic accuracy, with metastatic RCC cells commonly expressing markers such as CD10 and vimentin while harmful to cytokeratin 7 (CK7) [6,7]. This immune profile helps differentiate RCC metastases from other clear cell neoplasms and primary skin adnexal tumors. In this cases, a punch biopsy was performed to obtain a representative tissue sample. The most frequently reported immunohistochemical markers in RCC metastases are vimentin and CD10. A retrospective observational study conducted by Sutthiporn Namnak et al. determined that, in clear cell, papillary, and chromophobe renal cell carcinoma, CD10 was the most prominently expressed marker. Markers enhance diagnostic accuracy by distinguishing RCC metastases from other clear cell neoplasms and primary cutaneous tumors. Additionally, PAX8 has proven to be a valuable marker in diagnosing renal cell carcinoma (RCC), both in primary and metastatic tumors, PAX8 has high sensitivity and specificity, making it a reliable tool for distinguishing RCC from other types of neoplasms [17].
The prognosis for patients with cutaneous metastases from RCC is generally poor, reflecting advanced systemic disease [3,18]. The median survival after the appearance of skin metastases ranges from 6 to 10 months, although some patients may live longer depending on the disease burden and response to therapy [3]. Early detection of cutaneous metastases is essential, as it can prompt comprehensive staging to assess the extent of systemic involvement and guide therapeutic decisions.
Treatment options for metastatic RCC have evolved significantly with the introduction of targeted therapies and immunotherapies. Tyrosine kinase inhibitors (TKIs) such as sunitinib and pazopanib target angiogenesis pathways by inhibiting VEGF receptors, suppressing tumor growth and spread [13,19,20]. Immune checkpoint inhibitors, including nivolumab and pembrolizumab, target the PD-1/PD-L1 pathway, enhancing the immune system's ability to recognize and destroy tumor cells [12]. Combination therapies targeting multiple pathways have shown improved outcomes in some patients. However, responses can be variable, and treatment is often palliative, aiming to control symptoms and improve quality of life.
In the presented cases, initiating systemic therapy following the diagnosis of cutaneous metastases was crucial. The first patient began treatment with a TKI, leading to partial regression of the skin lesion. The second patient received immunotherapy, which may offer durable responses due to its mechanism of enhancing anti-tumor immunity. These cases illustrate the potential benefits of systemic therapies in managing metastatic RCC, although the overall prognosis remains guarded.
The occurrence of cutaneous metastases significantly impacts patient management. To ensure comprehensive care, we need a multidisciplinary approach involving dermatologists, oncologists, pathologists, and other specialists. Patient education is also vital; we should inform individuals with a history of RCC about the importance of monitoring for new or changing skin lesions and encourage them to seek prompt medical evaluation.
From a dermatological perspective, these cases highlight the critical role of dermatologists in the early detection of metastatic disease. Awareness of the varied presentations of cutaneous metastases and familiarity with dermoscopic features can facilitate timely diagnosis. Furthermore, collaboration with pathologists for histopathological and immunohistochemical analysis enhances diagnostic accuracy.
In summary, cutaneous metastases from RCC, while rare, represent an important clinical entity that signals advanced disease. The two cases underscore the diversity of dermatological manifestations and the challenges in diagnosis. A high index of suspicion, thorough clinical evaluation, and prompt biopsy of suspicious lesions are essential. Advances in systemic therapies offer hope for improved management, but early detection remains critical to optimizing patient outcomes. Ongoing research and heightened clinical awareness are necessary to improve the recognition and treatment of cutaneous metastases in RCC.
CONCLUSIONS
Clinicians should recognize that cutaneous metastases from renal cell carcinoma, as illustrated in these cases, serve as important indicators of advanced systemic disease. These metastases can present subtly, and clinicians often misdiagnose them, which delays crucial treatment. When evaluating new or unusual skin lesions in patients with a history of renal malignancy, clinicians should maintain a high index of suspicion for metastatic RCC. Prompt diagnosis through careful assessment and biopsy is essential for initiating appropriate systemic therapies. Early detection and a multidisciplinary approach can improve management strategies and potentially enhance patient outcomes.
CONFLICT OF INTEREST STATEMENT
The authors declare no conflicts of interest.
FUNDING SOURCES
No funding was received for this study.
AUTHOR CONTRIBUTIONS
Consent
Written informed consent was obtained from the patient for the publication of this case report and accompanying images.
REFERENCES
- Moch H, Gasser T, Amin MB, Torhorst J, Sauter G, Mihatsch MJ. (2000). Prognostic utility of the recently recommended histologic classification and revised TNM staging system of renal cell carcinoma: a Swiss experience with 588 tumors. Cancer. 89(3):604-614.
- Singh P, Somani K. (2020). Latent distant metastasis of renal cell carcinoma to skin: A case report. Clin Case Rep. 8(7):1138-1141.
- Silver E, Roudakova K, Bial N, Daniel D. (2021). Cutaneous Metastasis of Renal Cell Carcinoma to the Cheek: A Case Report and Literature Review. Am J Case Rep. 22:e928999.
- Amin A, Burgess EF. (2016). Skin manifestations associated with kidney cancer. Semin Oncol. 43(3):408-412.
- Posadas EM, Limvorasak S, Figlin RA. (2017). Targeted therapies for renal cell carcinoma. Nat Rev Nephrol. 13(8):496-511.
- Balawender K, Przybyła R, Orkisz S, Wawrzyniak A, Boroñ D, Grabarek BO. (2022). Cutaneous metastasis as the first sign of renal cell carcinoma - crossroad between literature analysis and own observations. Postepy Dermatol Alergol. 39(3):553-558.
- Namnak S, Kittikowit W, Wongphoom J. (2013). The role of immunohistochemistry in diagnosis of renal cell carcinoma subtypes. Asian Archives of Pathology. 9(1):9-16.
- Nabi S, Kessler ER, Bernard B, Flaig TW, Lam ET. (2018). Renal cell carcinoma: a review of biology and pathophysiology. F1000Res. 7:307.
- Lorenzo-Rios D, Cruzval-O'Reilly E, Rabelo-Cartagena J. (2020). Facial Cutaneous Metastasis in Renal Cell Carcinoma. Cureus. 12(12):e12093.
- Brownstein MH, Helwig EB. (1972). Metastatic tumors of the skin. Cancer. 29(5):1298-307.
- Dika E, Veronesi G, Ferroni L, Patrizi A, Campione E, Moliterni E, et al. (2020). Cutaneous metastases from renal cell carcinoma: A multicenter study. Melanoma Research. 30(2):187-192.
- Wen L, Guo L, Zhang W, Li Y, Jiang W, Di X, et al. (2019). Cooperation Between the Inflammation and Coagulation Systems Promotes the Survival of Circulating Tumor Cells in Renal Cell Carcinoma Patients. Front Oncol. 9:504.
- Wang B, Song JW, Chen HQ. (2020). First-Line Pazopanib Treatment in Metastatic Renal Cell Carcinoma: Real-World Data From a Single Chinese Center. Front Pharmacol. 11:517672.
- Agha RA, Franchi T, Sohrabi C, Mathew G, Kerwan A; SCARE Group. (2020). The SCARE 2020 Guideline: Updating Consensus Surgical CAse REport (SCARE) Guidelines. Int J Surg. 84:226-230.
- Alonso-de León T, Cano-Aguilar LE. (2023). Metástasis cutáneas diagnosticadas en un hospital de segundo nivel desde 1985 al 2020. Medicina Cutánea. 51(3):103-110.
- Gutiérrez Olivares VM. (2019). Perfil inmunohistoquímico de los tumores de células renales. Medicina Cutánea Ibero-Latino-Americana. 47(2):89-97.
- Barr ML, Jilaveanu LB, Camp RL, Adeniran AJ, Kluger HM, Shuch B. (2015). PAX-8 expression in renal tumours and distant sites: a useful marker of primary and metastatic renal cell carcinoma? J Clin Pathol. 68(1):12-17.
- Rosenthal A, McGrath D, Krajnik J, Langtry J. (2018). Cutaneous metastasis of renal cell carcinoma: A case report and review of the literature. Journal of Clinical Oncology. 36(15_suppl).
- Czarnecka AM, Brodziak A, Sobczuk P, Dendek C, Labochka D, Korniluk J, et al. (2019). Metastatic Tumor Burden and Loci as Predictors of First Line Sunitinib Treatment Efficacy in Patients with Renal Cell Carcinoma. Sci Rep. 9(1):7754.
- Sandock DS, Seftel AD, Resnick MI. (1995). A new protocol for the followup of renal cell carcinoma based on pathological stage. J Urol. 154(1):28-31.