2024: Volume 4, Issue 4
Past Issues
 Abstract
Abstract  PDF
PDFEfficacy of a Topical Serum Combined with a Sunscreen on Pigmented Macules of the Face and Neck: A Non-Randomized Clinical Trial on Dark Skin in Sub-Saharan Africa
Kourouma Hamdan Sarah1,2,*, Gbandama Koffi Kouamé Pacôme1,2, Nguena Feungue Ulrich1, Aminatou Adda Ngaoundéré1
1Dermatology department of the Hospital and University Center of Treichville, Abidjan, Ivory Coast
2University Félix Houphouet-Boigny, Abidjan, Ivory Coast
*Corresponding author: Kourouma Hamdan Sarah, Department of Dermatology and Venereology, Treichville University Hospital, Abidjan / University Felix Houphouët-Boigny, Cocody, Abidjan, Côte d'Ivoire, Tel: +225 07 07 72 59 82, ORCID: 0000-0002-9077-7010; Email: [email protected]
Received Date: August 19, 2024
Publication Date: August 29, 2024
Citation: Sarah KH, et al. (2024). Efficacy of a Topical Serum Combined with a Sunscreen on Pigmented Macules of the Face and Neck: A Non-Randomized Clinical Trial on Dark Skin in Sub-Saharan Africa. Dermis. 4(4):21.
Copyright: Sarah KH, et al. © (2024).
ABSTRACT
Introduction: The efficacy of chemical depigmenting agents on dark and very dark skin (phototypes IV to VI) remains poorly documented. Objective: This study aimed to evaluate the efficacy of a topical serum combined with a sunscreen on hyperpigmentation in a population with pigmented skin in sub-Saharan Africa. Methods: This was a non-randomized clinical study in a Dermatology-Venerology Department during 4 months. The patients included were over 18 years of age and presented with hyperpigmented macules on the face or neck. The protocol consisted of the application of a topical serum and a sunscreen to the face and neck. The efficacy of these products was assessed using a melanin index meter (MASI score). Results: Forty-six (46) women with dark phototypes (IV, V, VI) were included. The mean age was 33.8 ± 8.7 years (16-50 years). Hyperpigmentation after acne predominated (67.4%). Comparison of the mean hyperpigmentation index showed a significant difference (p<0.001). Comparison of the mean Healthy Skin Index showed that the Serum Booster significantly improved participants' skin tone at Day 30 and this improvement increased through to D90. A comparison of the participants' MASI scores showed significant differences from day 30 (p=0.001). The percentage efficacy of the combination used on patients' pigmented macules was 91.3%. A comparison of participants' quality of life showed a significant difference (p=0.001) at D90. Participants reported no side effects or signs of intolerance. Conclusion: This clinical trial showed the efficacy of a depigmenting agent and a sunscreen on hyperpigmentation of dark phototypes in Africa.
Keywords: Africa, Hyperpigmentation, Pigmented Skin, Pigmentation Disorders, Sun Protection Factor
INTRODUCTION
Hyperpigmented macules or hyperpigmentation are a common reason for dermatological consultation [1]. The most common aetiologies are lentigo, post-inflammatory hyperpigmentation, dark circles and melasma [2]. Treatment of cutaneous hyperpigmentation can include physical means such as laser, cryotherapy, peelings and depigmenting agents such as hydroquinone, azelaic acid, niacinamide, retinoic acid, ascorbic acid, arbutin [3]. Several clinical trials have demonstrated the efficacy of these different depigmenting agents on light phototypes (I to III) [4]. In darker phototypes, pigmented macules are more frequent and more severe and represent a greater aesthetic problem in dermatological consultations [1,5]. The efficacy of depigmenting agents in general and in darker phototypes in sub-Saharan Africa is poorly reported in the literature. The majority of research investigating the efficacy of depigmenting products on hyperpigmented macules has been conducted in Asian and Western countries [6]. However, no studies from Sub-Saharan Africa on this subject have been identified. In this context, we proposed to conduct a study on the efficacy of a combination of a hyperpigmentation correcting serum and a chemical sunscreen on hyperpigmentation in pigmented skin.
OBJECTIVE
This study aimed to evaluate the efficacy of a combination of a topical serum and a sunscreen on hyperpigmentation of the face and neck in a population with pigmented skin in Côte d'Ivoire (Sub-Saharan Africa).
METHODS
Type, scope of study and period: This was a non-randomized clinical study of 4 months. The study took place at the Dermatology-Venerology Department of the University Hospital Center (CHU) of Treichville in Abidjan. This institution is the main reference center for dermatology in Côte d'Ivoire.
Study population: Our source population consisted of all patients consulting the Dermatology-Venerology Department of the CHU of Treichville. The target population was all patients with hyperpigmented macules on the face and neck.
Inclusion criteria: Cases were defined as any person of dark phototype (IV-V-VI), over 18 years of age, presenting with post-inflammatory hyperpigmented macules (acne, pyoderma, or other), melasma, of post-traumatic origin, or other, and who gave informed consent.
Non-inclusion criteria: We did not include:
- Patients who had used anti-spot cream for hyperpigmentation of the face and neck in the 6 months prior to enrollment,
- Patients with allergy to any of the components of the serum and/or sunscreen,
- Patients undergoing systemic corticosteroid therapy, and
- Patients with severe exogenous ochronosis (associated with spontaneous skin depigmentation).
Exclusion criteria: After enrollment, any patient who experienced severe irritation or an adverse event related to the use of either product during the course of the study and any patient who decided to withdraw from the study during the course of the study were excluded.
Products used in the therapeutic protocol: The products used for the study were TOPICREM MELA Serum Booster and TOPICREM CALM+ soothing protective cream SPF 50+.
Sampling method: Sampling was consecutive and complete. Patients were consecutively enrolled in the study. All patients who met the selection criteria were retained until the minimum sample size was reached. The formula used to calculate the minimum sample size was that used in the experimental studies by Withney and Ball in 2002. A clinical study conducted by Alvin et al. in 2011 entitled "A comparative study of the safety and efficacy of 75% mulberry (Morus alba) extract oil versus placebo as a topical treatment for melasma: a randomized, single-blind, placebo-controlled trial" evaluated the effect of an antitache agent.
Sample size: The minimum sample size, calculated using the formula of Withley and Ball's experimental studies with an alpha threshold of 5% and a power of 80%, was 32 participants per group [7].
Data collection: A data collection form was used to collect sociodemographic data (age, sex, occupation, religion), clinical data (location of lesions, number of pigmented patches, causes of hyperpigmentation), and pigmentation intensity assessed with the mexameter® MX 18. It is a device that measures two essential components of the skin responsible for skin color: the amount of melanin and the amount of hemoglobin on a skin area of approximately 5 mm in diameter. The measuring principle is absorption/reflection. The meter emits 3 specific wavelengths. A receiver measures the amount of radiation reflected from the skin. The amount of energy absorbed by the skin defines the amount of melanin and hemoglobin, thus allowing to define a pigmentation score of the skin surface concerned. The mexameter has several indications, including measuring the effectiveness of anti-spot creams.
For this study, the mexameter was used to evaluate the Melasma Area and Severity Index (MASI) score for each patient. The Melasma Area and Severity Index (MASI), developed by Kimbrough-Green et al in 1994, was probably the first scoring system that attempted to objectively assess and measure the response of melasma to treatment in a clinical trial, taking into account both the area affected and the intensity of the melasma.
The quality of life of patients with pigmented macules has also been assessed using the Melasma Quality of Life Scale (MELASQOL). Balkrishnan et al. developed the MELASQOL in 2003 [8]. On a Likert scale ranging from 1 (not bothered at all) to 7 (bothered all the time), the subject rated how he/she felt.
The MELASQOL is scored from 7 to 70, with higher scores indicating poorer quality of life due to melasma.
The procedures in our study consisted of four visits as follows:
- 1st visit: Month 0 (inclusion)
Patients were interviewed about the interest of the study and its benefit; then their signed informed consent was obtained. If the patient met the selection criteria, the data collection form was administered. Then, the melanin index of the pigment spot (baseline melanin index) was measured with the MX18 mexameter and an iconography of the lesions was made with a Nikon® digital camera. The patient also completed the MELASQOL questionnaire. If the patient had several pigmented macules, the median melanin index was used. Each patient received 1 tube of a Serum Booster (quantity 30ml) and 1 tube of a sunscreen (quantity 40ml). These products were eventually renewed during subsequent visits. The application protocol for the Serum Booster and the sunscreen was well explained to the patient, also documented, and given to the patient (It is recommended that the serum booster be applied each night, covering the entire face, prior to bedtime. Similarly, the sunscreen should be applied each morning, following bathing, and before any exposure to UV radiation). Finally, the investigator's contact information was given to the patient to report any side effects, signs of intolerance or any additional explanations needed. A first appointment was made at M1 for the first evaluation.
- At the second visit, the patient's compliance with the treatment (especially with the application protocol) and the presence of side effects were checked. A second measurement of the melanin index (melanin index at D30) and photographs (from the same angle) were taken.
- The third visit consisted of measuring the melanin index at M2 (60 days), taking photos of the hyperpigmentation, verifying that the protocol had been properly followed, and looking for any side effects.
- The fourth visit consisted of measuring the melanin index at M3 (90 days), taking photos, checking that the protocol had been followed correctly, looking for any side effects and refilling the MELASQOL bottle.
The application protocol of the products was as follows
- The Serum booster: one application every evening on the pigmentation spots and on the whole face and neck;
- the sunscreen: one application every morning on the whole face and neck.
Data processing: The data collected were recorded in CSPRO 7.3 and then exported to SPSS version 26.0 for statistical analysis. Quantitative variables were expressed as their means with their standard deviations and extremes if their distribution followed a normal distribution. If the distribution of quantitative variables did not follow a normal distribution, they were expressed as their medians with their interquartile ranges and extremes. To evaluate the efficacy of the protocol, the mean melanin indices (MASI score) before and after treatment (M1, M2 and M3) were compared using Student's t-test if the distribution of the variables was normal. Otherwise, pre- and post-treatment melanin indices were compared using the Willcoxon Man Whitney U test. Categorical variables were expressed as numbers and percentages and compared using the chi-squared test or Fisher's test if any of the cells had an observed number less than 5. The significance level was set at 5%. We evaluate the Global Aesthetic Improvement (GAIS) for both the physicians and the participants.
Ethical Considerations: The study protocol that we developed was submitted and approved by the Ethics Committee of the University Hospital of Treichville before the start of the study. We also obtained the approval of the Director of the University Hospital of Treichville and the Head of the Department of Dermatology and Venereology before the start of the study. A verbal and signed informed consent was obtained from each participant before the start of the study. The anonymity of the patients was maintained; the study data and photographs taken will be used only for the purposes of this study. The study was conducted in accordance with the ethical standards of Helsinki.
RESULTS
We recruited 46 patients of dark phototype (IV, V, VI) with hyperpigmented macules on the face and/or neck; all were female. The predominant age range was 30 to 40 years (20 cases; 43.5%) (Figure 1). The mean age of the participants was 33.8 ± 8.7 years (16 and 50 years). The majority of participants were employed in the private sector (20 cases; 43.5%). The hyperpigmented macules of the patients were mainly post-acne (31 cases; 67.4%), followed by sun-exposure related macules (10 cases; %) and melasma (3 cases; 6.5%) (Table I). Comparison of the mean hyperpigmentation index from day 1 to day 30, day 60, and day 90 (Table II; Figure 2) showed a statistically significant difference (p<0.001) between the mean hyperpigmentation index at day 1 versus day 60 and versus day 90. In contrast, there was no statistically significant difference (p≥0.05) in the mean hyperpigmentation index at day 1 versus day 30. The comparison of the mean healthy skin indices on day 1, day 30, day 60 and day 90 (Table III; Figure 3) showed that the Serum booster significantly improved the skin tone of the participants on day 30 and that this improvement increased until day 90. Thus, the percentage efficacy of the combination of the Serum booster and the sunscreen on the pigmented macules of the patients from day 1 to day 90 was 91.3%. A comparison of the participants' MASI scores between day 1 and day 90 (Table IV; Figure 4) showed significant differences as early as day 30 (p=0.001). A comparison of participants' quality of life on Day 1 and Day 90 (Table V) showed a statistically significant difference at Day 90 (p=0.001). Using GAIS Assessment, physicians reported score 3 to score 2 (improved too much improved) representing 90% of participants. Participants, 42/46 (91%), showed at least a 1 score improvement. After two months of application of the products (D60), no side effects were reported and two patients reported a feeling of tightness (1 case; 2.2%) and very mild pruritus (1 case; 2.2%). After three months of using the products, participants reported no side effects or functional signs.
Table I. Etiologic diagnosis of Hyperpigmentation (n = 46)
|
Etiologic diagnosis |
Number (n) |
Percentage |
|
Acne |
31 |
67,4 |
|
Sun exposure |
10 |
21,8 |
|
Melasma |
3 |
6,5 |
|
Voluntary skin depigmentation |
2 |
4,3 |
|
Total |
46 |
100 |
Table II. Comparison of Average Hyperpigmentation indices from Day 1 to Day 30, Day 60 and Day 90
|
|
Average ± SD |
P value |
|
Comparison of hyperpigmentation index on Day 1 and Day 30 |
|
|
|
Index J1 |
738,5 ± 167,6 |
0,118 |
|
Index J30 |
710,0 ± 135,6 |
|
|
Comparison of hyperpigmentation index on Day 1 and Day 60 |
|
|
|
Index J1 |
738,5 ± 167,6 |
0,007 |
|
Index J60 |
687,6 ± 136,3 |
|
|
Comparison of hyperpigmentation index on Day 1 and Day 90 |
|
|
|
Index J1 |
738,5 ± 167,6 |
<0,001 |
|
Index J90 |
647,1 ± 143,4 |
|
Table III. Comparison of average healthy skin indexes at Day 1, Day 30, Day 60 and Day 90
|
|
Average ± SD |
P Value |
|
Comparison of healthy skin indexes on Day 1 and Day 30 |
|
|
|
Index J1 |
638,3 ± 140,0 |
0,011 |
|
Index J30 |
588,9 ± 157,0 |
|
|
Comparison of healthy skin indexes on Day 1 and Day 60 |
|
|
|
Index J1 |
638,3 ± 140,0 |
<0,001 |
|
Index J60 |
582,1 ± 135,6 |
|
|
Comparison of healthy skin indexes on Day 1 and Day 90 |
|
|
|
Index J1 |
638,3 ± 140,0 |
<0,001 |
|
Index J90 |
576,1 ± 137,6 |
|
SD: Standard Deviation
Table IV. Comparison of MASI at Day 1, Day 30, Day 60 and Day 90
|
|
Median(IQR) |
Valeur P |
|
Comparison of MASI Day 1 and Day 30 |
|
|
|
Index J1 |
5,5 (3,2 – 7,7) |
<0,001 |
|
Index J30 |
2,9 (1,7 – 5,0) |
|
|
Comparison of MASI Day 1 and Day 60 |
|
|
|
Index J1 |
5,5 (3,2 – 7,7) |
<0,001 |
|
Index J60 |
1,7 (0,9 – 3,8) |
|
|
Comparison of MASI Day 1 and Day 90 |
|
|
|
Index J1 |
5,5 (3,2 – 7,7) |
<0,001 |
|
Index J90 |
0,9 (0,6 – 1,6) |
|
IQR: interquartile range MASI: Melasma Area and Severity Index
Table V. Comparison of Quality of Life on Day 1 and Day 90
|
|
Median(IQR) |
P value |
|
Quality of life |
|
|
|
Index J1 |
24,0 (14,8 – 34,0) |
<0,001 |
|
Index J90 |
16,0 (11,8 – 23,3) |
|
IQR: Interquartile Range
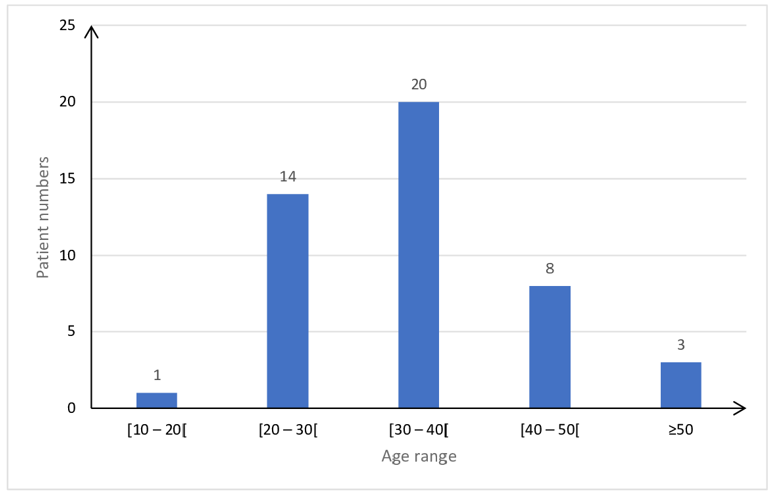
Figure 1. Distribution of parents by age group (n=46).
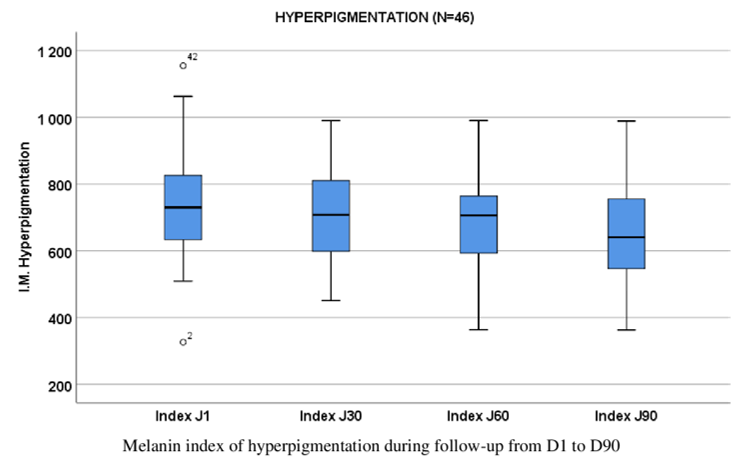
Figure 2. Box plots of melanin indices of hyperpigmentation from day 1 to day 90 (n = 46).
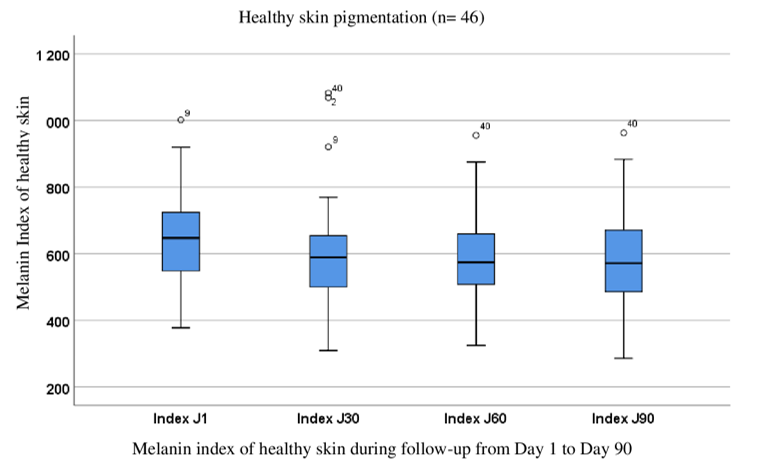
Figure 3. Box plots of melanin indices of healthy skin from Day 1 to Day 90 (n = 46).

Figure 4. Evolution of the appearance of pigment macules in a participant from month 0 to month 3.
DISCUSSION
This study evaluated the efficacy of the combination of a Serum booster and a sunscreen on hyperpigmented macules of the face and neck in dark phototype patients living in sub-Saharan Africa. The difficulties we faced were related to patients being late for their appointments and having to be called back each time for their appointments. However, we were able to follow all patients according to the established protocol and obtain usable data. Hyperpigmented macules are more common in patients with darker phototypes and are a real concern for them, potentially affecting their quality of life [9]. Very often, peri- and post-inflammatory hyperpigmentation is the most visible consequence of acne and leads patients to minimize acne treatment [10]. These hyperpigmentations lead patients to seek solutions to make them disappear, which leads them to turn to cheap products sold by people with no proven scientific qualifications. All subjects in this study were female. Dégboé et al. [11] in Benin also found a predominance of women in their study (72.9%) [11]. Women, in contrast to men, are more concerned about any changes related to their health in general, but even more so about the health and beauty of their skin. Given the conspicuous nature of facial macular pigmentation, the need for treatment is higher in women. For the majority of our participants who worked in the private sector, having a flawless face was an imperative, as for some they were the face of their company to clients. According to Briganti et al, there are many methods to attenuate pigmentary macules [12]. The safest and most effective method is to inhibit melanin production by blocking the key enzyme, tyrosinase [13,14]. The combination of depigmenting agents has been shown to be more effective on pigmented macules than a single depigmenting agent. The Serum Booster contains as main ingredients: a complex nonapeptide (decrease of melanin production), a vitamin C derivative, ascorbyl glucoside (decrease of melanin synthesis), vitamin PP or niacinamide (decrease of melanin transfer). All of these ingredients are known to have different depigmenting actions that, when put together, present a notable effectiveness on hyperpigmentation [15]. Several authors have demonstrated these lightening effects of vitamin C and vitamin PP [16-18]. In addition, the addition of a cream with a sun protection factor was justified by the prevention of the occurrence and aggravation of pigmented macules on black skin.
There was a statistically significant difference between the average hyperpigmentation index on day 1 compared to day 60 and compared to day 90 (p=0.001) with an efficacy percentage of 91.3%. These results showed that Serum Booster in combination with the sunscreen resulted in a significant reduction of macular hyperpigmentation from day 60 of treatment. On healthy skin, the combination of Serum Booster with sunscreen improved skin radiance as early as day 30 after the start of application. Participants reported an improvement in their quality of life after three months of using the products. Very few side effects and functional signs were reported from day 1 to day 90. All these data confirmed the efficacy of the products in improving the participants' appearance and thus their quality of life. In addition, the products were well tolerated by the participants' skin. This good tolerability of the products used by the patients was related to certain ingredients of the sunscreen, namely the unsaponifiable matter of sunflower seed oil and phytic acid. Sunflower seed oil is known to maintain the integrity of the stratum corneum and improve hydration of adult skin without inducing erythema [19]. Phytic acid is an antioxidant derived from grains, legumes and rice. Formulated at 2%, it is soothing and has exfoliating and brightening properties [20].
CONCLUSION
This non-randomized clinical study tested the efficacy of the combination of an anti-staining product (Serum Booster) and a chemical sunscreen on hyperpigmented macules in dark phototype individuals in Africa. The results allowed us to note that this combination presented a remarkable efficacy on hyperpigmentation about 91.3% and a good tolerance in the users.
ACKNOWLEDGEMENTS
The authors would like to thank the Nigy Topicrem Group for their support in the practical implementation of this study.
CONFLICT OF INTEREST
The authors received financial and material support from the Nigy Topicrem Group for the study and publication of the data.
MAYOLY SPINDLER Laboratories has patented the combination of depigmenting agents in TOPICREM MELA Serum Booster.
REFERENCES
- Makino ET, Huang P, Cheng T, Acevedo SF, De Oliveira C, Mehta RC. (2023). 12-Week, single-center study of a targeted Pigment-Correcting Dark Spot Treatment for Post-Inflammatory Hyperpigmentation and Solar lentigines. Clin Cosmet Investig Dermatol. 16:2677-2686.
- Rossi AB, Leyden JJ, Pappert AS, Ramaswamy A, Nkengne A, Ramaswamy R, et al. (2011). A pilot methodology study for the photographic assessment of post-inflammatory hyperpigmentation in patients treated with tretinoin. J Eur Acad Dermatol Venereol. 25(4):398-402.
- Ortonne JP. (2008). Traitement des hyper et des hypomélanoses. In: Dermatologie et infections sexuellement transmissibles. 5e éd. Paris: Elsevier-Masson. 9-4. p. 464‑466.
- Navarrete-Solís J, Castanedo-Cázares JP, Torres-Álvarez B, Oros-Ovalle C, Fuentes-Ahumada C, González FJ, et al. (2011). A Double-Blind, Randomized Clinical Trial of Niacinamide 4% versus Hydroquinone 4% in the Treatment of Melasma. Dermatol Res Pract. 2011:379173.
- Davis EC, Callender VD. (2010). Postinflammatory hyperpigmentation: a review of the epidemiology, clinical features, and treatment options in skin of color. J Clin Aesthet Dermatol. 3(7):20-31.
- Roohaninasab M, Mojtabaee M, Livani F, Heidari N, Alizadeh N, Khosravi S. (2022). Beneficial esthetic lightening effects of Cuscuta extract on skin darkness in healthy individuals: A clinical trial study. J Family Med Prim Care. 11(11):6890-6895.
- Alvin G, Catambay N, Vergara A, Jamora MJ. (2011). A comparative study of the safety and efficacy of 75% mulberry (Morus alba) extract oil versus placebo as a topical treatment for melasma: a randomized, single-blind, placebo-controlled trial. J Drugs Dermatol. 10(9):1025-1031.
- Balkrishnan R, McMichael AJ, Camacho FT, Saltzberg F, Housman TS, Grummer S, et al. (2003). Development and validation of a health-related quality of life instrument for women with melasma. Br J Dermatol. 149(3):572-577.
- Boukari F, Jourdan E, Fontas E, Montaudié H, Castela E, Lacour JP, et al. (2015). Prevention of melasma relapses with sunscreen combining protection against UV and short wavelengths of visible light: a prospective randomized comparative trial. J Am Acad Dermatol. 72(1):189-190.e1.
- Fitoussi C. Acné sur peau noire. [Consulté le 08 Août 2022]. Réalités thérapeutiques en Dermato-Vénérologie. Publié le 12 Décembre 2017. Disponible sur : https://www.realites-dermatologiques.com/2017/12/acne-sur-peau-noire/
- Dégboé BE, Koudoukpo C, Agbéssi N, Akpadjan F, Adégbidi H, Atadokpèdé F. (2019). Acné sur peau noire : facteurs associés et comorbidités psychiatriques dans les services de dermatologie du Bénin. Ann Dermatol Venereol. 146(12, Supplement):A205-A206.
- Briganti S, Camera E, Picardo M. (2003). Chemical and instrumental approaches to treat hyperpigmentation. Pigment Cell Res. 16(2):101-110.
- Espín JC, Varón R, Fenoll LG, Gilabert MA, García-Ruíz PA, Tudela J, et al. (2000). Kinetic characterization of the substrate specificity and mechanism of mushroom tyrosinase. Eur J Biochem. 267(5):1270-1279.
- García-Molina F, Hiner AN, Fenoll LG, Rodríguez-Lopez JN, García-Ruiz PA, García-Cánovas F, et al. (2005). Mushroom tyrosinase: catalase activity, inhibition, and suicide inactivation. J Agric Food Chem. 53(9):3702-3709.
- Rendon M, Horwitz S. (2012). [Topical treatment of hyperpigmentation disorders]. Ann Dermatol Venereol. 139(Suppl 3):S102-S107.
- Al-Niaimi F, Chiang NYZ. (2017). Topical Vitamin C and the Skin: Mechanisms of Action and Clinical Applications. J Clin Aesthet Dermatol. 10(7):14-17.
- Chiu PC, Chan CC, Lin HM, Chiu HC. (2007). The clinical anti-aging effects of topical kinetin and niacinamide in Asians: a randomized, double-blind, placebo-controlled, split-face comparative trial. J Cosmet Dermatol. 6(4):243-249.
- Hakozaki T, Minwalla L, Zhuang J, Chhoa M, Matsubara A, Miyamoto K, et al. (2002). The effect of niacinamide on reducing cutaneous pigmentation and suppression of melanosome transfer. Br J Dermatol. 147(1):20-31.
- Danby SG, AlEnezi T, Sultan A, Lavender T, Chittock J, Brown K, et al. (2013). Effect of olive and sunflower seed oil on the adult skin barrier: implications for neonatal skin care. Pediatr Dermatol. 30(1):42-50.
- Houshmand EB. (2021). Effect of glycolic acid, phytic acid, soothing complex containing Emulsion on Hyperpigmentation and skin luminosity: A clinical evaluation. J Cosmet Dermatol. 20(3):776-780.