2024: Volume 4, Issue 5
Past Issues
 Abstract
Abstract  PDF
PDFHuman Recombinant Growth Factors and Their Effect on Vaginal Microbiota Modulation in Menopause Patients
Pablo González-Isaza1,*, Diana Velez Rizo2
1Department of Obstetrics & Gynecology, Hospital Universitario San Jorge, Colombia
2Department of Gynecology, La Cardio, Bogotá DC, Colombia
*Corresponding author: Pablo González-Isaza, MD, Department of Obstetrics & Gynecology, Hospital Universitario San Jorge, Cra. 4 # 24-88, Pereira, Risaralda, Colombia, Phone: 320.788.7509, ORCID: 0000-0001-7798-5141; Email: [email protected]
Received Date: December 09, 2024
Publication Date: December 20, 2024
Citation: González-Isaza P, et al. (2024). Human Recombinant Growth Factors and Their Effect on Vaginal Microbiota Modulation in Menopause Patients. Dermis. 4(5):26.
Copyright: González-Isaza P, et al. © (2024).
ABSTRACT
Genitourinary syndrome of menopause (GSM) is a normal consequence of aging, hormonal deprivation, or cancer treatments, it is estimated to affect approximately 1 out of 2 women. Management of symptoms has limited benefit. Restoration of a healthy vaginal microbiome may be an ideal avenue for management of GSM. The purpose of this study was to evaluate the effect of a novel topical formulation of human recombinant growth factors on vaginal microbiota modulation in menopause patients. A prospective single center longitudinal study included 37 voluntary patients with symptoms related to GSM and dysbiosis, such as vaginal discharge and odor. A home-based regimen of human recombinant growth factors was used by patients twice a week, up to follow up at six months. Evaluations included validated questionnaires, punch biopsies and vaginal swabs performed at baseline, and at the end of the study period. Vaginal flora modulation and normal pH were achieved by the end of the treatment protocol. Topical human recombinant growth factors to modulate vaginal microbiota are a viable alternative therapy for GSM.
Keywords: Menopause, Genitourinary Syndrome of Menopause, Vaginal Microbiota, Vaginal Microbiome, Growth Factors
ABBREVIATIONS
GSM: Genitourinary Syndrome of Menopause.
INTRODUCTION
Genitourinary syndrome of menopause (GSM) is a normal consequence of aging, hormonal deprivation, or cancer treatments, it is estimated to affect approximately 1 out of 2 women [1]. The most frequent symptoms are related to vaginal dryness and dyspareunia. Traditional treatments such as vaginal moisturizers may be of limited benefit, and relief of symptoms can be inconsistent or limited as well due to hyperosmotic properties of most compounds available on the market [2]. Genital and urological complications such as urinary infections and vaginitis are related to alkaline pH, leading to the replacement of normal, healthy vaginal microbiota by pathogenic anaerobic bacteria [3]. The ovulatory cycle also influences vaginal microbiota, affected by the action of estrogen and progesterone on the vaginal epithelium, due to an increase in thickness and glycogen production.
Lactobacillus population alteration is common in 50% of post-menopausal women with higher serum levels of follicle-stimulating hormone and lower estrogen levels [4]. Available treatments are targeted to improve dryness and dyspareunia, but few reports on the management of vaginal microbiota dysbiosis are available inside the scientific literature, mostly because there is a poor understanding of the pathophysiological scenario of a healthy vaginal environment.
Vaginal microbiota dysbiosis can be treated with oral hormone replacement therapy and vaginal probiotic therapies [5]. In a previous report we demonstrated clinical and histological improvement of vaginal atrophy inside a group of patients treated with human recombinant growth factors [6]. Other alternatives include isoflavone gel, applied to a group of 103 women biweekly for 12 weeks, with reportedly statistically significant improvement in vaginal health and pH acidification [7]. On the other hand, the use of thermal therapies such as fractional CO2 laser showed not only a reduction of clinical symptoms but positive changes in vaginal microbiota due to a remodeling status in vaginal epithelium and modulation of inflammatory cytokines, without adverse effects [8]. Panyawongudom, et al. found no statistically significant difference in vaginal lactobacilli grading before and after treatment with Er:YAG laser as compared with a sham procedure [9]. Newer approaches such as the use of highly purified polynucleotides from trout gonads seemingly demonstrate regenerative properties for the treatment of vulvovaginal atrophy and vulvar fissures [10].
The main objective of this investigation is to evaluate the microbiological changes related to the vaginal microbiome in post-menopausal women, before and after a regimen of topical human recombinant growth factors, and to evaluate the improvement of symptoms related to vaginal atrophy, sexual health, and quality of life.
MATERIALS AND METHODS
A prospective, single center longitudinal study was performed from March to October 2023, with patients meeting inclusion criteria from urogynecology and minimally invasive surgery department of obstetrics and gynecology, Hospital Universitario San Jorge, Pereira, Colombia. Inclusion and exclusion criteria are summarized in Table 1. A total of 37 women (mean age 58.3 years) were included in the study group. Patients recruited for this study were volunteers from the urogynecology unit. Informed consent was obtained along with written authorization, included in their medical records according to the Helsinki declaration, Belmont report, CIOMS rules, GPC/ICH and the 008430 resolution of the Colombian government (stabilized on 4th October 1993). Ethics Committee from epidemiology unit, Hospital Universitario San Jorge, Pereira, Colombia, considered the study as minimal risk or beyond minimal risk as follows:
- Adjust and briefly explain the ethical principles that warrant investigation according to international standards.
- Based on previously conducted experiments on animals in laboratories and other scientific facts that show a secure intervention in humans.
- Clearly express the risks and security guarantees to participants.
- Having the written informed consent of research subjects or their legal representative.
- Relate the experience of researchers and the responsibility of a health entity.
Initial consultation included physical examination and the completion of vulvovaginal symptoms questionnaire (VVSQ) (11). Visual analog scale at baseline, 3 months and 6 months, vaginal swabs were sent for a microbiological analysis to evaluate Maturation index (MI), values ≤ 49 means no estrogenic effect on cells; 50–64 denotes moderate estrogenic effect on cells, and 65–100 is related to a more dominant estrogenic environment [12]. Vaginal microbiome was also evaluated using Nugent Score where 0-3=normal, 4-6-=intermediate, and 7-10=defined as dysbiosis or bacterial vaginosis [13].
One sachet of human recombinant growth factors was used intravaginally at night twice a week during the study protocol.
The software used for the statistical analysis was Epi Info (Centers for Disease Control, Atlanta, GA., USA), using the 2x2 table and Chi square tests in the statistical calculator to obtain p value, with the exposures and outcomes prospectively. The variables analyzed via software included Nugent Score, the VVSQ (Vulvovaginal Symptom Questionnaire), and vaginal pH.
Table 1. Inclusion and Exclusion Criteria
|
INCLUSION CRITERIA |
EXCLUSION CRITERIA |
|
Age 45-80 |
History of vaginal surgeries |
|
Amenorrhea >12 months |
Use of local hormone therapy 6 months previous |
|
Vaginal dryness |
Genital prolapse any compartment > POP-Q 2 |
|
Entry dyspareunia |
History of pessary use |
|
Secondary sexual dysfunction |
Patient not sexually active |
|
History of vulvar fisures |
Urodynamic urinary incontinence |
|
History of more than three episodes of vaginal infection with vaginal discharge and odor |
Mental illness |
|
No previous pharmacological treatments |
Bed prostration, diaper use |
|
No previous treatment via energy-based devices (Laser, Radiofrequency, HIFU) |
Vaginal stenosis TVL < 4 cm |
RESULTS
No adverse events were found during the development and follow-up of the study. Table 2 summarizes the overall results of this investigation.
Improvement in symptoms was reported by all subjects from the beginning to the end of the study, with a statistically significant overall p value, consistent with agreement with the primary end point. By positively modulating the vaginal microbiota, the genitourinary symptoms of each patient would improve, including symptoms of dryness secondary to vaginal atrophy. Vaginal pH at the end of the follow-up in each of these volunteers decreased, confirming that modulation of the microbiota is decisive for having a better vaginal microenvironment, allowing physicians to preserve and restore genitourinary function and reduce incidence of symptoms. VMI questionnaire scores also presented a statistically significant improvement (p=0.02) at 6-month follow-up.
Changes in VVSQ score over the course of the study were statistically significant (p=0.04). This variable correlates with the primary end point of this study since the intervention carried out with human growth factors in volunteers showed improvement in genitourinary symptoms at the end of the 6-month follow-up, and the other variables studied outside of vaginal dryness were also improved.
Variable NS (NUGENT SCORE) evaluates the vaginal microbiome of each patient, in which all participants presented vaginal dysbiosis at follow-up. The overall p value was 0.07; although there is no statistical significance, 14 of these patients went on to experience an intermediate state and the other 20 improved their vaginal microbiota.
Table 2. Study Results by Visit
|
Scores |
Visit 1 |
Visit 2 12 weeks |
Visit 3 24 weeks |
P Value |
ODOR BASELINE |
ODOR END |
|
VVSQ |
16.1 +/- 2.1 |
10.48 +/- 2.1 |
7.4 +/- 0.70 |
0.04 |
YES |
NO |
|
VMI |
48.44 +/- 45.3 |
57.86 +/- 14.1 |
65.89 +/- 14.1 |
0.02 |
|
|
|
Nugent Score |
7.0 +/- 1.4 |
4.8 +/- 0.70 |
3.2 +/- 0.71 |
0.07 |
|
|
|
pH |
6.5 +/- 0.22 |
|
4,97 +/- 0.18 |
0.03 |
|
|
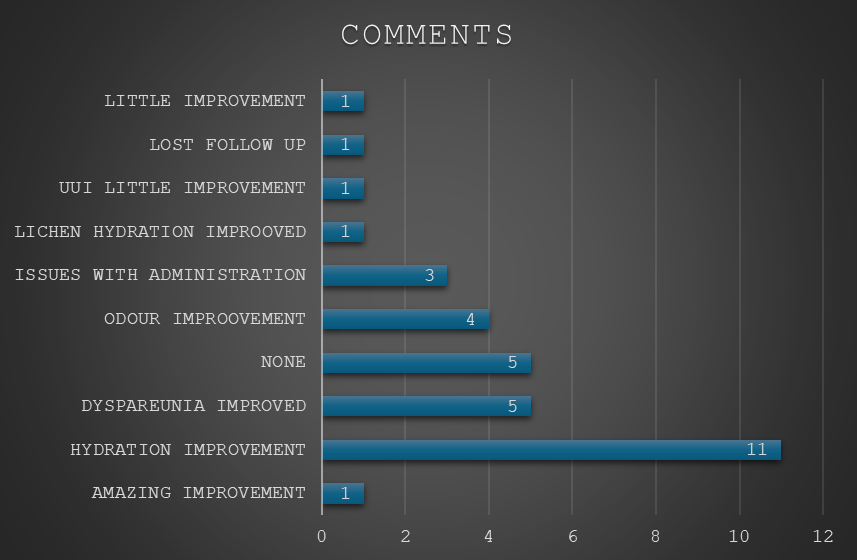
Figure 1. Summary of Patient Comments About Symptoms.
DISCUSSION
The main objective of this study was to demonstrate that the use of recombinant human growth factors has a positive effect on the modulation of the vaginal microbiota in menopausal women, and to reaffirm the improvement of vaginal dryness in atrophic vulvovaginitis observed in the literature. Subjects evaluated had similar demographic characteristics, making them suitable for inclusion in the study. Methodology included volunteers with symptoms related to the genitourinary syndrome of menopause due to the presence of vulvovaginal atrophy and vaginal dysbiosis.
Nowadays there is consistent evidence of the microbiological characteristics of the vaginal environment in the different stages of a woman’s life. Post-menopausal symptoms include genitourinary deterioration with vaginal dryness and atrophy being the most annoying, with secondary dysbiosis leading to recurrent vaginal infections and constant discomfort. Regarding the alteration in the lactobacilli population, Hummelen and colleagues described a clear relationship between greater vaginal bacterial diversity and low population of lactobacilli with complaints of vaginal dryness. It is clear that local hormone therapy can affect the vaginal microbiota and reduce pH; compared to moisturizing creams, there was no evidence on its role in acidifying vaginal pH or modulating the microbiota [14]. The management of microbiota dysbiosis can impact urogenital health because lactobacilli are considered important biomarkers of vaginal homeostasis, and there is a close relationship between hormonal levels and the population of lactobacilli. Shen et al. [4] also considered that hormonal status governs glycogen availability at the level of the vaginal epithelium, which is an important substance for the survival of lactobacilli [15].
In the era of regenerative medicine, it is important to offer women alternatives that can have a significant impact on symptoms of GSM such as vulvovaginal atrophy, vaginal dryness and reduced homeostasis of the microbiota. A recent systematic review reported that the use of topical hyaluronic acid and glycerin for vaginal atrophy was safe and effective [16]. The topical use of recombinant human growth factors follows the principles of regenerative medicine. While it has already been proven to be a safe hormonal alternative for vaginal atrophy, this is the first report of its kind that also found a significant improvement in the population of lactobacilli such as a direct sign of modulation of the vaginal microbiota.
Of note, this study yielded positive comments from each of the patients regarding the symptoms they presented at the beginning of the study, and the positive changes they experienced at final follow-up, described in Graph 1. The topical growth factor intervention given generated an improvement in the microbiome, with the outcomes classified by each patient as satisfactory and a positive improvement in their quality of life.
Further study would include a larger population with a long follow-up, and to have a control group for comparison, to confirm and support the findings of this investigation.
CONCLUSION
The relationship between the microbiome and postmenopausal vulvovaginal symptoms seems to be related to the bacterial vaginal population. The vaginal microbiome has different characteristics at different stages of the female reproductive and post reproductive life cycle. Gonadal hormone levels (progesterone and estrogen) were also different at these times. Fluctuations in progesterone and estrogen levels in the female vaginal epithelium and the availability of glycogen may influence the composition and diversity of the vaginal microbiota. The growth factor intervention given positively influenced this composition, resulting in satisfactory and positive for the improvement in each subject’s quality of life. Thus, the human growth factors are a viable alternative to improve the balance of the vaginal microbiome and subsequently, the symptoms of vulvovaginal atrophy in the postmenopausal population.
REFERENCES
- Portman DJ, Gass ML. (2014). Genitourinary syndrome of menopause: new terminology for vulvovaginal atrophy from the International Society for the Study of Women’s Sexual Health and the North American Menopause Society. Menopause. 21(10):1063-1068.
- Management of symptomatic vulvovaginal atrophy: 2013 position statement of the North American Menopause Society. Menopause. 20(9):888-904.
- Gandhi J, Chen A, Dagur G, Suh Y, Smith N, Cali B, Khan SA. (2016). Genitourinary syndrome of menopause: an overview of clinical manifestations, pathophysiology, etiology, evaluation, and management. Am J Obstet Gynecol. 215(6):704-711.
- Shen L, Zhang W, Yuan Y, Zhu W, Shang A. (2022). Vaginal microecological characteristics of women in different physiological and pathological period. Front Cell Infect Microbiol. 12:959793.
- Muhleisen AL, Herbst-Kralovetz MM. (2016). Menopause and the vaginal microbiome. Maturitas. 91:42-50.
- Isaza PG. (2019). Use of Growth Factors for Vulvo/Vaginal Bio-Stimulation. Surg Technol Int. 34:269-273.
- Chaudhary D, Mishra V, Chaudhary S, Rajender G. (2023). A prospective study to investigate the 12-week efficacy of soy isoflavone vaginal gel (0.5%) in postmenopausal women with symptoms of vulvovaginal atrophy. J South Asian Feder Obs Gynae. 15(3):308-312.
- Becorpi A, Campisciano G, Zanotta N, Tredici Z, Guaschino S, Petraglia F, et al. (2018). Fractional CO2 laser for genitourinary syndrome of menopause in breast cancer survivors: clinical, immunological, and microbiological aspects. Lasers Med Sci. 33(5):1047-1054.
- Panyawongudom N, Panyakhamlerd K, Suwan A. (2023). Number of vaginal lactobacilli in postmenopausal women with vaginal atrophy before and after treatment with erbium-YAG laser: a randomized sham-controlled trial. BMC Womens Health. 23(1):513.
- Valenti P, Rosa L, Capobianco D, Lepanto MS, Schiavi E, Cutone A, et al. (2018). Role of Lactobacilli and Lactoferrin in the Mucosal Cervicovaginal Defense. Front Immunol. 9:376.
- Erekson EA, Yip SO, Wedderburn TS, Martin DK, Li FY, Choi JN, et al. (2013). The Vulvovaginal Symptoms Questionnaire: a questionnaire for measuring vulvovaginal symptoms in postmenopausal women. Menopause. 20(9):973-979.
- Lindau ST, Dude A, Gavrilova N, Hoffmann JN, Schumm LP, McClintock MK. (2017). Prevalence and correlates of vaginal estrogenization in postmenopausal women in the United States. Menopause. 24(5):536-545.
- Amegashie CP, Gilbert NM, Peipert JF, Allsworth JE, Lewis WG, Lewis AL. (2017). Relationship between nugent score and vaginal epithelial exfoliation. PLoS One. 12(5):e0177797.
- Stabile G, Topouzova GA, De Seta F. (2023). The role of microbiota in the management of genitourinary syndrome of menopause. Climacteric. 26(4):353-360.
- Palacios S. (2020). Non-hormonal approaches for the treatment of vulvovaginal atrophy: the choice between hyaluronic acid and glycerin. Gynecol Endocrinol. 36(10):847-848.
- Buzzaccarini G, Marin L, Noventa M, Vitagliano A, Riva A, Dessole F, et al. (2021). Hyaluronic acid in vulvar and vaginal administration: evidence from a literature systematic review. Climacteric. 24(6):560-571.