2024: Volume 4, Issue 3
Past Issues
 Abstract
Abstract  PDF
PDFKeloids from Ear Piercing in People with Pigmented Skin in Sub-Saharan Africa: Modalities and Complications
Kourouma Hamdan Sarah*, Gbandama Koffi Kouamé Pacôme, Allou Ange-Sylvain, Amani Kaunan Leslie-Wilfried Gbonangbo, Coulibaly Souleymane Aziz, Kouassi Yao Isidore, Kouassi Kouamé Alexandre, Ahogo Kouadio Célestin, Kouamé Kanga, Kaloga Mamadou, Ecra Elidjé Joseph, Gbery Ildevert Patrice, Sangaré Abdoulaye
Department of Dermatology and Venereology, Treichville University Hospital, Abidjan / University Felix Houphouët-Boigny, Cocody, Abidjan, Côte d'Ivoire
*Corresponding author: KOUROUMA Hamdan Sarah, Department of Dermatology and Venereology, Treichville University Hospital, Abidjan / University Felix Houphouët-Boigny, Cocody, Abidjan, Côte d'Ivoire; Email: [email protected]; ORCID number: 0000-0002-9077-7010
Received Date: April 25, 2024
Publication Date: May 7, 2024
Citation: Sarah KH, et al. (2024). Compare the Keloids from Ear Piercing in People with Pigmented Skin in Sub-Saharan Africa: Modalities and Complications. Dermis. 4(3):20.
Copyright: Sarah KH, et al. © (2024).
ABSTRACT
Introduction: Ear piercing, a practice for aesthetic or ritual purposes, exposes practitioners to infectious and allergic risks. On pigmented skin, the risk of the appearance of a keloid scar should be noted. Our objective is to study piercing modalities and complications, factors favoring keloids, and clinical aspects on dark skin. Methodology: Cross-sectional study carried out over a year, in the dermatology department of the Treichville University Hospital (Abidjan), including adult patients of dark phototypes, presenting a post-piercing keloid of the ear. Results: Seventy-two patients were recruited, giving a hospital prevalence of 0.96% of post-ear-piercing keloids. And a proportion of 39% among keloids of all locations. Women represented 92% (sex ratio of 0.4). The average age was 25.61±5.77 years {18 – 52}. Thirty-six percent (36%) had a family history of keloids. The average time to onset after piercing was 14.9 months. It was mainly done at home (56%) and with jewelry (82%). The ear lobule was the main site (61%) with a single keloid in 90% of patients. Post-piercing skin infections were present in 53%. Surgical ablation followed by corticosteroid infiltration was the main treatment performed (77%). Carrying out the piercing at home (p<0.001), the use of jewelry for piercing (p=0.002), the large size of keloids (p=0.002), poor aseptic conditions (p<0.001) were statistically linked to the occurrence of keloids. Conclusion: Ear piercing at home, the use of jewelry, the large size of keloids, and poor aseptic conditions could promote the appearance of ear keloids on pigmented skin in sub-Saharan Africa.
Keywords: Piercing; Ear Keloid; Pigmented Skin; Africa
INTRODUCTION
Keloid scars are benign fibrous skin tumors that originate from the reticular dermis [1]. They can occur spontaneously or as a result of infection or skin trauma, particularly following piercing, and are more common in patients with a personal and/or family history of keloids [2-6]. Piercings are body modifications that involve perforating the ear or another part of the body to insert an ornament for aesthetic or ritual purposes, depending on the culture [7]. The practice of piercing carries risks of infection and allergic reactions due to the conditions and metals used. Additionally, there is a risk of keloid scarring at the site of the piercing, which is more common in individuals with darker skin pigmentation [8]. The study aimed to describe piercing modalities and complications, factors favoring keloids, and clinical aspects on dark skin in tropical Africa.
MATERIAL AND METHODS
Type and scope of the study: This was a descriptive and analytical cross-sectional study conducted at the Dermatology and Venereology Department of Treichville University Hospital.
Study Period: January to December 2021, a period of twelve months.
Study population: The study population consisted of individuals of any sex aged 18 or over who exhibited keloid scarring of the ear.
Inclusion criteria: Patients aged 18 and above with keloid scars of the ear, regardless of sex, who have provided their informed consent to participate in the study. The diagnosis of keloid was based on the following criteria:
- Scar of hard consistency
- Evolving for more than 12 to 18 months beyond the limits of the lesion, with no tendency to regress
- Pruritic and irregular, with or without pain
- Presence of crab-leg expansion
Non-inclusion criteria: Patients with hypertrophic scars were not included.
Data Collection: The data were collected via a survey form following questioning and a clinical examination of patients seen in consultation at Treichville University Hospital.
Data processing: The data were processed and analyzed anonymously using SPSS 21 software. Tables, graphs, and figures were produced using Excel 2016 and Word 2016. Quantitative variables were expressed as mean ± standard deviation or median and were compared using Student or Wilcoxon tests. Categorical variables were expressed as headcount (percentages) and were compared using chi-square or Fisher tests. The significance level was set at 5%.
Ethical Considerations: The study was submitted for approval to the Medical and Scientific Director of the Treichville Hospital and University Center, which acts as the local ethics committee. The data collected did not identify the patients included in the study. The patients provided their verbal and signed consent for the use of the data collected in a scientific publication.
RESULTS
Socio-professional Characteristics of Patients
During the study period, 7508 patients consulted the clinic, including 185 cases of keloid scars in various locations, resulting in a prevalence of 2.46%. Out of these cases, 72 were ear keloids, accounting for 38.92% of all keloids and a hospital prevalence of 0.96%. The study population was predominantly female (92%), with a sex ratio (M/F) of 1:11. The mean age of patients was 25.61 ± 5.77 years [18-52], with a predominance of patients aged between 18 and 25 years. All patients had phototype VI. Out of the total number of patients, 55 (76%) had a higher level of education, with the majority being pupils and students (55%). Table 1 summarizes the socio-demographic characteristics of the patients.
Table 1: Main socio-demographic characteristics of patients with keloids.
|
Characteristics |
Effectives |
Percentage |
|
Age range [18 – 25 years [ |
33 |
46 |
|
Gender Female Male |
66 06 |
92 08 |
|
Occupation Students |
40 |
55 |
|
Education level University |
55 |
76 |
|
Monthly income < 60000 FCFA [300000 – 450000 FCFA[ |
39 05 |
54 07 |
FCFA: French African Colonies Francs
Clinical Features of Keloid Scars
The mean age of patients at the time of piercing was 21.90 ± 5.03 years (extremes 13 and 41 years). There was a personal (39%) and family (36%) history of keloid scarring. The average time to keloid formation after piercing was 14.87 ± 5.10 months (07 and 24 months). Pruritus was the most frequent functional symptom, present in 70 patients (97%). Keloid scars were located preferentially in the ear lobules (61%) (Figure 1) and averaged between 2 and 6 cm in size (Table 2).
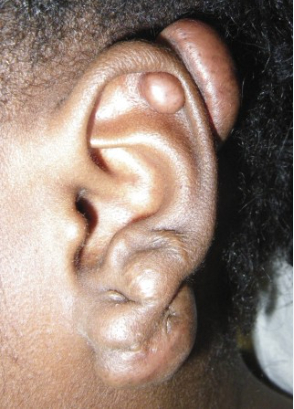
Figure 1: Post-piercing keloid scar of the left ear in a 35-year-old adult woman.
Table 2: Distribution of patients according to keloid characteristics.
|
Characteristics of keloids |
Effectives (n=72) |
Percentage |
|
Siege Helix Anthelix Lobula |
34 03 44 |
47 04 61 |
|
Count 1 2 3 |
65 05 02 |
90 07 03 |
|
Size Small Medium Large |
13 35 24 |
18 49 33 |
|
Skin condition Normal Hyperpigmented Hypopigmented |
03 66 03 |
04 92 04 |
The conditions under which ear piercings were performed and the post-piercing procedures are summarized in Tables 3 and 4.
Table 3: Distribution of patients by piercing method (n= 72).
|
Piercing procedures |
Effectives |
Percentage |
|
Reason for design Mode Aesthetics Culture |
55 11 06 |
77 15 08 |
|
Place of realization Home Market Professional Institute |
40 18 14 |
56 25 19 |
|
Material for piercing Pistol Disposable piercing needle Sewing needle Piercing catheter Jewelry |
04 02 04 03 59 |
06 03 06 04 82 |
|
Aseptic conditions Alcohol Others |
28 24 04 |
39 33 06 |
Table 4: Distribution of patients according to post-piercing modalities (n=72).
|
Post-piercing procedures |
Effectives |
Percentage |
|
Number of piercings performed 1 2 3 or more |
05 59 08 |
07 82 11 |
|
Type of jewelry worn With pressure With loop Broom Wire |
25 42 03 02 |
35 58 04 03 |
|
Complications Infection Ulceration |
45 29 38 |
62 40 53 |
Treatment of Keloids
Of the total number of patients, 35 (49%) received keloid scar treatment. Surgery was the most common treatment, with 27 patients (77%) undergoing this procedure. Intracheloidal infiltration was the second most common treatment, with 7 patients (20%) receiving it, followed by pressure therapy, which was used on only 1 patient (3%).
Analytical study
No statistically significant association was found between age, reason for piercing, place of piercing, number and complications of piercing, and number of ear keloids (refer to Table 5).
Table 5: Characteristics by age of piercing.
|
Variables |
≤ 25 years n = 56 ; (%) |
> 25 years n = 16 ; (%) |
p-value |
|
Reason for design Mode Aesthetics Culture |
45 (80) 07 (13) 04 (07) |
10 (63) 04 (25) 02 (12) |
0,329 |
|
Place of realization Home Market Professional Institute |
32 (57) 15 (27) 09 (16) |
08 (50) 03 (19) 05 (31) |
0,385 |
|
Number of ear piercings 1 2 3 or more |
02 (04) 47 (84) 07 (12) |
03 (19) 12 (75) 01 (06) |
0,096 |
|
Complications Yes No |
36 (64) 20 (36) |
09 (56) 07 (44) |
0,558 |
|
Number of ear keloids 1 2 3 |
51 (91) 03 (05) 02 (04) |
14 (88) 02 (12) 00 (00) |
0,472 |
However, a statistically significant association was observed between the place of piercing (p<0.001), use of inappropriate jewelry (p= 0.002), large keloid size (> 6cm) (p= 0.002), and occurrence of post-piercing complications (refer to Table 6).
Table 6: Characteristics according to the occurrence of complications.
|
Variables |
Onset of complications |
p-value |
|
|
Yes n = 45 ; (%) |
No n = 27 ; (%) |
||
|
Aseptic conditions Yes No |
12 (27) 33 (73) |
16 (59) 11 (41) |
0,006
|
|
Place of realization Home Market Professional Institute |
30 (67) 13 (29) 02 (04) |
10 (37) 05 (19) 12 (44) |
< 0,001
|
|
Type of jewelry worn after piercing With pressure With loop Other |
09 (20) 31 (69) 05 (11) |
16 (59) 11 (41) 00 (00) |
0,002
|
|
Number of ear keloids 1 keloid At least 2 keloids |
39 (87) 06 (13) |
26 (96) 01 (04) |
0,180
|
|
Size of keloids on the ear Small Medium Large |
04 (09) 20 (44) 21 (47) |
09 (33) 15 (56) 03 (11) |
0,002
|
DISCUSSION
This study aimed to describe keloid scars of the ear after piercing in phototype VI patients.
Our study found a higher frequency of keloids (38.92%) compared to Kassi et al. (4.9%, 2016) in our same department, Allah et al. (25.5%, 2013) in Abidjan, and Traoré et al. (8.8%, 2019) in Ouagadougou [9-11]. However, it was lower than the findings of Carmassi et al. in France, who reported 38 cases of keloids, including 44.4% of ear keloids [12]. This increase may be associated with the growing prevalence of piercings among the Ivorian population.
The observed average age (25.61 ± 5.77 years) was slightly higher than that reported by Kluger et al. in France (20.6 years for men and 18.9 years for women) [13]. The prevalence of piercing decreased with age, with the phenomenon mainly affecting the 16-24 age group in the Kibadi study in Congo [14]. These data were compared with hospital statistics, which showed a predominance of keloids in young subjects in the immediate post-pubertal period (between 16 and 30 years of age). This period is characterized by significant hormonal changes [14]. Additionally, some authors have suggested that the high incidence of keloids in young subjects was due to increased skin tension, while older subjects experienced skin slackening [15].
Niang et al. (2015) in Senegal and Kassi et al. (2012) in Côte d'Ivoire have also highlighted the predominance of female piercings [16, 9]. Although piercings are mainly for aesthetic purposes, they are more common among women in our regions [14]. However, our series also included five men who were interested in piercings. In their 2012 study in Antananarivo, Ahn et al. (2012) also found piercings among men [17].
Kibadi et al. (2017) conducted a study in the Democratic Republic of Congo (DRC) and reported a high prevalence of keloids among students (65.7%), which is higher than the prevalence found in our study (55%) [14]. The study suggested that the importance of physical appearance and the desire to follow fashion trends through mimicry may lead young people to use ornamental objects such as ear jewelry.
A study conducted in Burkina Faso in 2019 found that 22.4% of patients had a family history of keloids, a figure slightly lower than our findings of 36% [2]. In contrast, only 2.3% of patients in the DRC had a family history of pathological scarring [14].
The earlobe was the most common site for ear piercings, while Kibadi et al. found the helix to be the preferred site in their study in the DRC (98.3%) [14]. Guiard-Schmid reported that jewelers still perform the majority of piercings, particularly of the ear lobes [18].
The average duration of keloid evolution was 14.87 ± 5.10 months, which is comparable to the results of the study by Kibadi et al. In their study, 132 patients (76.7%) had lesions that were at least one year old, and 40 patients (23.3%) had lesions that were less than one year old [14]. In Burkina Faso, Traoré et al. found an average lesion evolution time of 3.69 years [1 month - 17 years] in their study of keloids and hypertrophic scars in schools [2]. The time between injury and keloid formation varies. Keloids typically develop during the healing process and can appear within the first 12 months, although in some cases they may not appear for several years [1].
Pruritus was observed in 97% of the patients, which is comparable to the findings of Traoré et al.'s study in Burkina Faso, where pruritus was noted in 46 pupils [2]. Keloid scars can cause itching, pain (burning sensation), contact paresthesia, and a pulling sensation due to the continuous production of cells and the consequent increase in local pressure [1]. These symptoms usually are indicative of scar progression [16].
Reasons for getting piercings are primarily driven by fashion (75%) and aesthetics (15%). This is consistent with previous studies, such as Kibadi et al., who found that participants' motivations for getting a piercing were primarily aesthetic [14]. Kluger et al. also reported that the main motivations for getting piercings were to beautify the body (53.1%) and to distinguish oneself from others (31.1%) [13]. The young population in our country is often influenced by the fashion choices of their idols, who are frequently sports or music stars. It is important to note that this statement is subjective and should be marked as such.
Jewelry was the most commonly used piercing material for 79% of the patients. In the Democratic Republic of Congo, Kibadi et al. reported that the ear was pierced with the stem of the jewelry [14]. Khanna et al. in England stated that the most commonly used techniques were needle or gun piercing [20]. The inaccessibility of these sophisticated techniques to young adults in Africa could explain why they do their piercing at home, more simply with jewelry.
The high incidence of skin complications can be attributed to piercings being performed outside of specialized institutes and aseptic measures not being respected. This observation was also made by Kibadi et al. in their study, where patients had their piercings done in markets by sellers of costume jewelry. Local skin infections were the most frequent complication in our patients. The study conducted by Kluger et al. in France found that complications included infections (44%), healing problems (37.9%), skin irritation (29.7%), and itching (15%) [13]. Pathological scarring occurred after an allergic reaction or local inflammation in the Kibadi study [14]. Literature reports have documented ear complications after piercing [6, 21]. According to studies, ear piercing can result in complications ranging from minor infections to allergic reactions, keloid formation, or ear lobule tearing. Our study found that complications related to the piercing were linked to poor technique, poor jewelry quality, and failure to observe aseptic conditions. These factors were statistically associated with the occurrence of these complications.
Surgery was also used as a main method to treat keloids in the patients received. Keloids were treated using various therapeutic procedures in the Kibadi study conducted in the DRC, including intralesional corticosteroid infiltration, surgery (intra-cicatricial excision), pressotherapy, and silicone gel application [14]. In a previous study in Abidjan, Kassi et al. found that the triple combination of keloid excision, delayed corticosteroid infiltration, and pressotherapy was more effective in 95% of patients [9].
CONCLUSION
Post-piercing keloids of the ear are increasingly common in Abidjan hospitals, particularly among young women who follow fashion trends. These keloids are localized to the lobule and are often complicated by infections. Factors associated with the occurrence of keloids in the ear after a piercing include poor piercing technique, low-quality jewelry, and failure to observe aseptic conditions, all of which increase the risk of infection. To decrease the occurrence of these complications, it appears necessary to increase awareness and modify the behavior of young individuals who engage in this practice.
CONFLICT OF INTEREST
The authors declare no conflict of interest.
REFERENCES
- Philandrianos C, Kerfant N, Jaloux Jr C, Martinet L, Bertrand B, Casanova D. (2016). Les cicatrices chéloïdes (première partie): une pathologie de la cicatrisation cutanée. Ann Chir Plast Esthet. 61(2):128–135.
- Traoré A, Korsaga/Somé N, Zoungrana/Ouédraogo A, Zongo N, Tapsoba GP, Ouédraogo M et al. (2019). Keloids and hypertrophic scars in secondary school in the city of Ouagadougou (Burkina Faso). Our Dermatol Online. 10(e):e32.1-e32.8.
- Marneros AG, Norris JE, Olsen BR, Reichenberger E. (2001). Clinical genetics of familial keloids. Arch Dermatol. 137(11):1429–1434.
- English RS, Shenefelt PD. (1999). Keloids and hypertrophic scars. Dermatol Surg. 25(8):631–638.
- Omo-Dare P. (1975). Genetic studies on keloid. J Natl Med Assoc. 67(6):428-432.
- Bloom D. (1956). Heredity of keloids; review of the literature and report of a family with multiple keloids in five generations. N Y State J Med. 56(4):511–519.
- Wohlrab S, Stahl J, Kappeler PM. (2007). Modifying the body: Motivations for getting tattooed and pierced. Body Image. 4(1):87–95.
- Gauglitz GG, Korting HC, Pavicic T, Ruzicka T, Jeschke MG. (2011). Hypertrophic scarring and keloids: pathomechanisms and current and emerging treatment strategies. Mol Med. 17:113–125.
- Kassi K, Kouame K, Choaken G, Kouassi K, Allou A, Gbery IP et al. (2016). P 103 : Chéloïde de l’oreille chez le noir Africain : facteurs de risque et prise en charge thérapeutique. Ann Dermatol Venereol. 143(4, suppl 1):S69.
- Allah KC, Yéo S, Kossoko H, Assi Djè Bi Djè V, Kadio MR. (2013). Cicatrices chéloïdes sur peau noire : mythe ou réalité. Ann Chir Plast Esthet. 58(2):115-122.
- Traoré A, Korsaga/Somé N, Zoungrana/Ouédraogo A, Zongo N, Tapsoba GP, Ouédraogo/Ouédraogo M et al. (2019). Keloids and hypertrophic scars in secondary school in the city of Ouagadougou (Burkina Faso). Our Dermatol Online. 10(e):e32.1-e32.8.
- Carmassi M, Eraud J, Gonelli D, Magalon G, Meyer LA. (2015). Cicatrices chéloïdes : étude d’une série de cas. Ann Pathol. 35(2):148-153
- Kluger N, Misery L, Seité S, Taieb C. (2017). Les piercings corporels: étude épidémiologique sur un échantillon représentatif de 5000 français. Ann Dematol Venereol. 144(12, suppl):S234–S235.
- Kibadi K. (2021). Deuxième piercing auriculaire à but esthétique et apparition de cicatrices pathologiques chez les négroïdes : à propos de 172 observations dans une zone endémique de chéloïdes. Ann Chir Plast Esthet. 66(1):42–51.
- Rockwell WB, Cohen IK, Ehrlich HP. (1989). Keloids and hypertrophic scars: a comprehensive review. Plast Reconstr Surg. 84(5):827–837.
- Niang SO, Sankale AA, Fall F, Diallo M, Dieng MT, Kane A, et al. (2009). La place de la chirurgie dans la prise en charge des chéloïdes à Dakar. Med Afr Noire. 56(4):224–226.
- Ahn R, Rmj R, Mmra M, Np R, Ah R, Fa R. (2012). Prise en charge des chéloïdes d’oreilles au Centre Hospitalier Universitaire D’ANTANANARIVO. 31–40. Disponible sur : http://cidst.recherches.gov.mg/IMG/pdf/3med31-40.pdf
- Guiard-Schmid JB, Picard H, Slama L, Maslo C, Amiel C, Pialoux G et al. (2000). [Piercing and its infectious complications. A public health issue in France]. Presse Med. 29(35):1948-56.
- Kassi K, Ecra E, Kouame K, Kouassi A, Yoboue P, Kanga J. (2006). Profil épidémiologique et clinique des cicatrices chéloïdes. Guinée Med. 52:57-62.
- Khanna R, Kumar SS, Raju BS, Kumar AV. (1999). Body piercing in the accident and emergency department. J Accid Emerg Med. 16(6):418–21.
- Friedrich L, Madrid C, Odman-Jaques M, Yersin B, Carron PN. (2014). Complications liées aux piercings. Rev Med Suisse. 10(422):662–668.