2024: Volume 4, Issue 1
Past Issues
 Abstract
Abstract  PDF
PDFPathergy Phenomenom: Indicator of Recurrent Vegetative Pyoderma Gangrenosum
Mariel Pimentel Isa 1,*, Lina Pichardo Di Vanna2, Manuel Cochón Aranda3, Priscilla De Los Santos4, Lauri Moscoso4, Fernanda Nanita de Estévez5
1Department of Dermatology and Venerology, Dominican Dermatology Institute “Dr. Huberto Bogaert Diaz”, Dominican Republic
2Department of Pathology, Dominican Dermatology Institute “Dr. Huberto Bogaert Diaz”, Dominican Republic
*Corresponding Author: Dra. Mariel Amelia Isa Pimentel, Dominican Dermatology Institute “Dr. Huberto Bogaert Diaz”; Albert Thomas Ave #66, Santo Domingo 10306, Dominican Republic; Tel: +1 (809) 707-1245; Email: [email protected]
Received Date: February 28, 2024
Publication Date: March 30, 2024
Citation: Isa M, et al. (2024). Pathergy Phenomenom: Indicator of Recurrent Vegetative Pyoderma Gangrenosum. Dermis. 4(1):11.
Copyright: Isa M, et al. © (2024).
ABSTRACT
Background: Pyoderma gangrenosum vegetans is an uncommon subtype of pyoderma gangrenosum of unknown etiology. It manifests as a solitary superficial vegetative ulcer, usually on the head, neck, and trunk of gradual onset with good response to treatment with immunomodulators. Case report: A 65-year-old female patient, hypertensive, with a painful erythematous plaque of 2.5cm in diameter, with raised edges and a slightly depressed center with the presence of purulent collection on the dorsum of the right hand of 3 days of evolution. Skin biopsy showed dense and diffuse neutrophil infiltrates in dermis. The lesion showed spontaneous remission without treatment. One year later the patient presented a painful exulcerated erythematous plaque, with vegetative edges, with the presence of a serohematic crust on its surface, 10cm in diameter, with 15 days of evolution, on the same extremity. Patient reports similar injuries in the past that appear after being traumatized by rose thorns in her garden. Skin biopsy shows neutrophilic infiltrate. Topical steroid treatment was initiated with complete resolution of the lesion. Conclusion: Pyoderma gangrenosum vegetans is not associated with systemic diseases, showing a favorable prognosis. This patient meets the necessary criteria to make the diagnosis, presenting neutrophilic infiltrate in the biopsy, decrease in the lesion after treatment with steroids, Pathergy phenomenon, as well as absence of infection demonstrated by negative cultures (3).
Keywords: Pyoderma gangrenosum vegetans, Pathergy phenomenon, neutrophilic dermatosis
INTRODUCTION
Pyoderma gangrenosum (PG) is a rare clinical-pathological entity classified within the group of neutrophilic dermatoses, which exacerbates in up to 30% of cases with the Pathergy phenomenon [1]. Vegetative pyoderma gangrenosum (VPG) is an unusual subtype with unknown etiology, although immune system dysregulation has been proposed. It typically presents as a solitary superficial vegetative ulcer usually on the head, neck, and trunk with a gradual onset, responding well to treatment with topical or systemic immunomodulators, which confers a favorable prognosis [1,2].
CASE REPORT
A 65-year-old female presented with a 3-day history of a painful lesion on the dorsum of the right hand. Examination was notable for well circumscribed erythematous plaque of 2.5cm in diameter with raised borders and a slightly depressed center with purulent collection (Figure 1). The patient reported similar lesions occurring in the past after injuring herself with rose thorns from her garden. Histopathological study showed dense and diffuse infiltrate predominantly of neutrophils occupying the entire papillary and reticular dermis, accompanied by extravasated erythrocytes and discrete eosinophils (Figure 2A and B), considering Sweet syndrome as the main differential diagnosis. Moreover, mycological studies were suggested to rule out atypical lesions of sporotrichotic chancre. Additionally, she presented neutrophilia and elevated acute phase reactants. The lesion spontaneously resolved without any treatment (Figure 3), so no further studies were performed. A year later, she returned to the consult for presenting a 15-day history of a painful lesion in the same location as the previous year. On examination, there was an erythematous ulcerated plaque with vegetative borders and serohemorrhagic crust on its surface, 10cm in diameter (Figure 4). Biopsy was taken from the edge of the lesion, revealing an erosion covered by fibrin and neutrophils, as well as slight edema in the epidermis. Fibrin was observed in the upper dermis, with presence of neutrophils and extravasated erythrocytes (Figure 5A and B), with histopathological diagnosis of Vegetative Variant Pyoderma Gangrenosum. Routine laboratory tests showed no pathological alteration, except for elevated acute phase reactants (erythrocyte sedimentation rate and C-reactive protein), and neutrophilia in the complete blood count. Tumor markers and cultures for fungi and mycobacteria were negative. The patient was evaluated by the Gastroenterology and Gynecology departments, with no evidence of pathological findings. Given the single lesion and absence of systemic symptoms, topical treatment with 0.1% mometasone furoate cream twice daily for 15 days was initiated, with complete resolution of the lesion (Figure 6).

Figure 1: Clinical image of an erythematous plaque with raised edges and a depressed center.
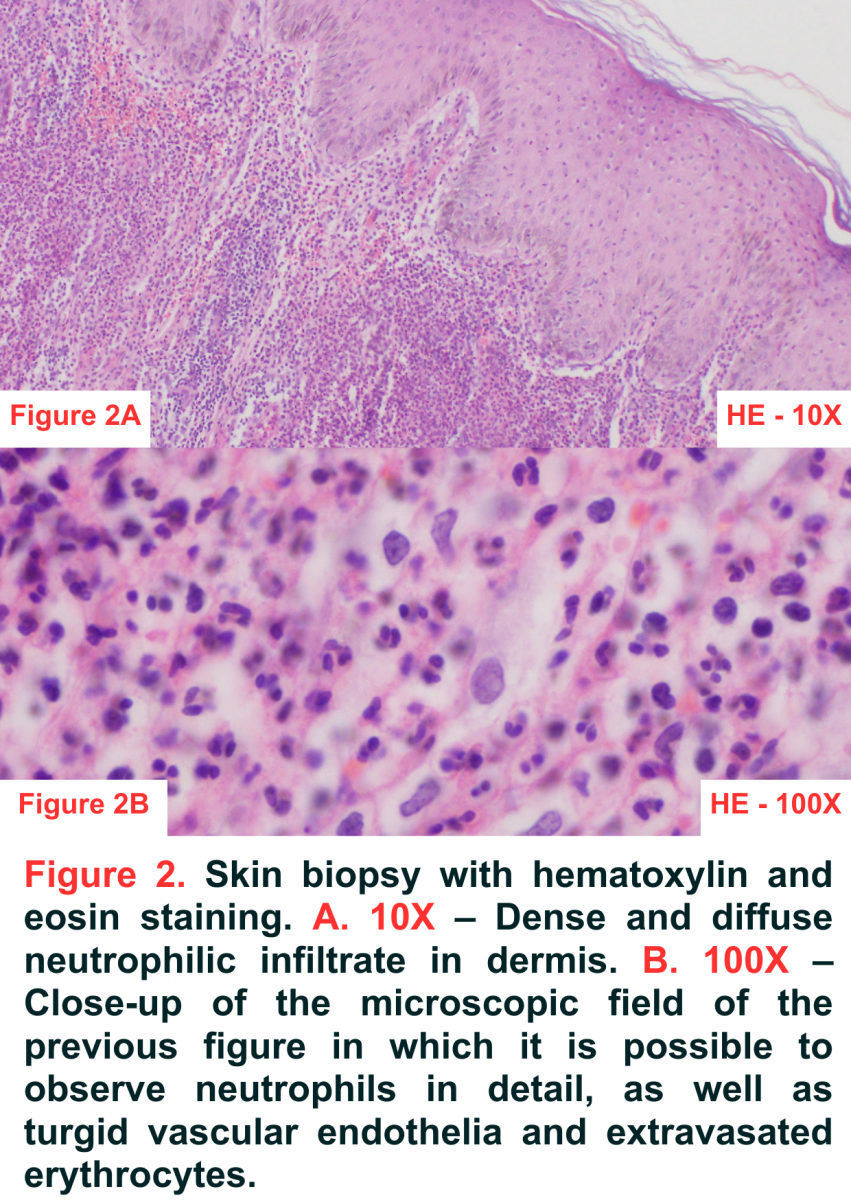
Figure 2: Skin biopsy with hematoxylin and eosin staining. A. 10X – Dense and diffuse neutrophilic infiltrate in dermis. B. 100X – Close-up of the microscopic field of the previous figure in which it is possible to observe neutrophils in detail, as well as turgid vascular endothelia and extravasated erythrocytes.

Figure 3: Remission of lesion with post-inflammatory hyperpigmentation.

Figure 4: Clinical image of an erythematous plaque exulcerated with vegetative edges and serohematic crust.
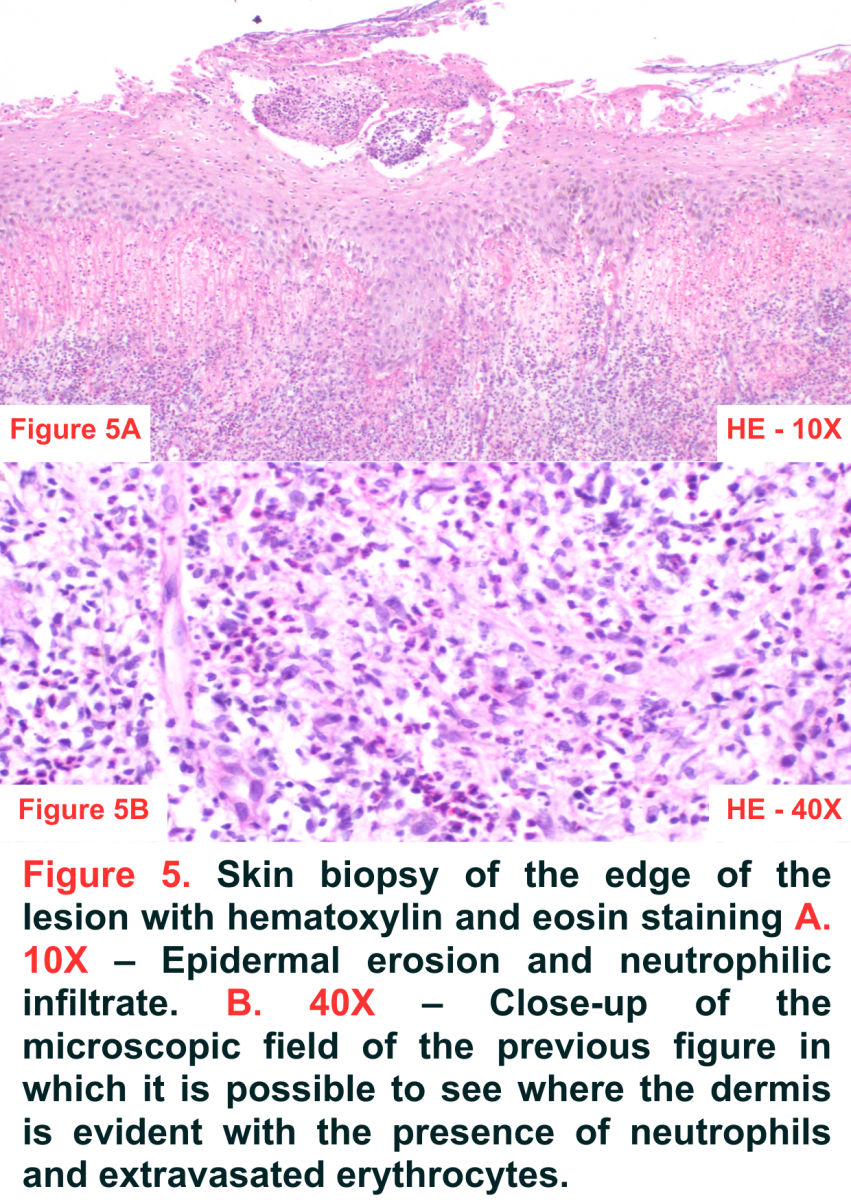
Figure 5: Skin biopsy of the edge of the lesion with hematoxylin and eosin staining A. 10X – Epidermal erosion and neutrophilic infiltrate. B. 40X – Close-up of the microscopic field of the previous figure in which it is possible to see where the dermis is evident with the presence of neutrophils and extravasated erythrocytes.

Figure 6: Hyperpigmented plaque with diffuse edges after treatment with medium-strength topical steroids.
DISCUSSION AND CONCLUSION
Among the variants of PG, the vegetative subtype is very uncommon. Unlike other subtypes of PG, it is not associated with systemic diseases, has a more indolent course, and tends to respond better to treatment compared to other variants, conferring a favorable prognosis [4]. Spontaneous healing is not rare, although recurrences are frequent [5] as in our patient, who had spontaneous remission in the first episode and subsequently experienced recurrences over the time.
PG is considered to have an immunological basis, based on a favorable response to immunomodulators, as well as the fact that it shows an exaggerated inflammatory reaction to various stimuli, as occurs in the Pathergy phenomenon, which induces or exacerbates PG in sites of minimal trauma [6] such as in our patient, who developed lesions after injuring herself with rose thorns from her garden.
The diagnosis of this pathology is made through clinical and histopathological findings, although this entity is a diagnosis of exclusion. There is a variety of histopathological findings of this pathology, depending on the stage of the lesion at which the biopsy is taken. An early lesion presents neutrophilic folliculitis and perifolliculitis, and intradermal neutrophilic abscess formation, while later lesions can show epidermal ulceration, superficial dermal necrosis, mixed inflammation with undermining at ulcer edge (characteristic) and abscess, leukocytoclastic vasculitis, and acanthosis in perilesional zone. Vegetative variant can show a reactive epidermal proliferation, dermal abscess, sinus tracts and palisading granulomas [2,5].
Corticosteroids are the first-line treatment. When the lesions are localized, the use of high-potency corticosteroids and topical calcineurin inhibitors is preferred. In cases of disseminated disease or treatment refractoriness, systemic corticosteroids or cyclosporine are opted [3]. In this case, we applied medium potency steroids in our patient, with satisfactory response and lower likelihood of side effects, with no recurrence.
The features that distinguish this pathology from classic PG include its lower association with systemic diseases and the good response to conservative treatments. The prognosis of PGV is very good, with a tendency towards complete healing [7].
REFERENCES
- Soto Vilches F, Vera-Kellet C. (2017). Pioderma gangrenoso: terapias clásicas y emergentes. Med Clin (Barc).
- Pizzariello G, Olivares L, Lois M, Anaya J, Maronna E. (2012). Pioderma gangrenoso vegetante. Presentación de 7 casos. Dermatol Argent. 18:383-388.
- Schroder M, Perez Search GC, SorinSearch I, Mazzuoccolo L. (2015) ‘Pyoderma gangrenosum vegetans. J ClinCase Rep. 5(11).
- Suárez-Pérez JA, Herrera-Acosta E, López-Navarro N, Vilchez-Márquez F, Prieto JD, Bosch RJ, et al. (2012). Pioderma gangrenoso: Presentación de 15 Casos Y revisión de la literatura, Actas Dermo-Sifiliográficas. 103(2):120–126.
- Ávila-López VH, Navarrete-Solís J, Hernández-Martínez SJ. (2021). Pioderma gangrenoso: características clínicas e histopatológicas de pacientes de una unidad de tercer nivel del noreste de México. Dermatol Rev Mex. 65 (2):149-158.
- Ormaechea-Pérez N, López-Pestaña A, Lobo-Morán C, Tuneu-Valls A. (2013). Pioderma granulomatoso superficial. Presentación de 2 casos tratados con tacrolimus tópico. Actas Dermo-Sifiliográficas. 104(8):721–724.
- Thomas KS, Ormerod AD, Craig FE, Greenlaw N, Norrie J, Mitchell E, et al. (2016). Clinical outcomes and response of patients applying topical therapy for pyoderma gangrenosum: A prospective cohort study. J Am Acad Dermatol. 75(5):940–949.