2024: Volume 4, Issue 1
Past Issues
 Abstract
Abstract  PDF
PDFPlatelet-Rich Plasma Therapy for Telogen Effluvium: A Comprehensive Evaluation of Efficacy and Safety
Uzma Dost Muhammad Rajar1*, Amin Fahim2, Sumayya Qazi3, Navaid Kazi4, Neeta Maheshwary5, Arjumand Ahmed- Rph6
1Department of Dermatology, Isra University Hyderabad, Pakistan
2Department of Pathology, People's University of Medical and Health Sciences for women, Isra University, Hyderabad, Pakistan
3Department of Biochemistry, Isra University Hyderabad, Pakistan
4Department of Physiology, Isra University Hyderabad, Pakistan
5Head of Medical Affairs, Helix Pharma, Karachi, Pakistan
6Medical Affairs, Helix Pharma, Karachi, Pakistan
*Corresponding Author: Uzma Dost Muhammad Rajar, Department of Dermatology, Isra University Hyderabad, Pakistan; Email: [email protected]
Received Date: February 26, 2024
Publication Date: March 20, 2024
Citation: Rajar UDM, et al. (2024). Platelet-Rich Plasma Therapy for Telogen Effluvium: A Comprehensive Evaluation of Efficacy and Safety. Dermis. 4(1):9.
Copyright : Rajar UDM, et al. © (2024).
ABSTRACT
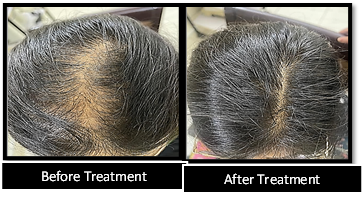
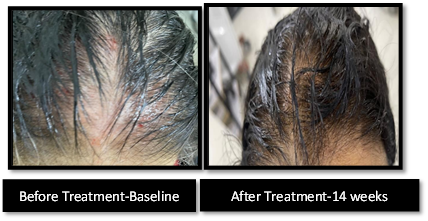
Background: Chronic Telogen Effluvium (TE) is a common hair loss condition. This study explores the effectiveness of PRP and Tressfix Serum in treating Chronic TE. It aims to uncover potential therapeutic approaches through microRNA expression analysis. Objective: The objective is to evaluate the effectiveness and safety of combining platelet-rich plasma (PRP) with Tressfix Serum in treating chronic TE and to evaluate the impact on microRNA expression related to this condition. Methods: Patients including both male and females of aged between 20-40 years diagnosed with TE were included. Patients with scalp-specific dermatological illnesses, such as psoriasis or seborrheic dermatitis, were excluded. PRP was prepared using a double spin process and injected intradermally at designated scalp sites. Patients underwent a total of seven treatment sessions over a 14-week period Results: The study demonstrated a significant improvement in hair regrowth and reduction in hair shedding among participants following PRP therapy. All miRNA expression was significantly reduced in group A and group B where as in group C five out of nine miRNA expresses no significant p>0.05 mean difference. The expression levels of hsa-mir-223 were considerably lower in Group A (PRP and Tressfix serum combined) (113.53±2.95) compared to Group B (PRP alone, 140.21±5.56) and Group C (Tressfix serum alone, 163.22±2.37). The expression of hsa-mir-212 was also less in Group A (53.5±7.56) than in Group B (75.58±8.71) and Group C (87.12±6.9). These variations in expression imply that the combination strategy of PRP and Tressfix serum may have a more significant impact on lowering microRNA expression linked to TE than either therapy alone. Conclusion: The study underscores the importance of patient selection criteria and meticulous technique in optimizing treatment outcomes. Further research is warranted to elucidate the long-term efficacy and durability of PRP therapy in TE management.
Keywords: MicroRNAs, Platelet-Rich Plasma (PRP), Scalp, Telogen effluvium (TE), SALT scale
INTRODUCTION
Telogen effluvium (TE) is a kind of hair loss that is more frequent in women and is generally caused by a combination of causes such as stressful events, trauma, hormonal imbalance, sickness, malnutrition and certain medicaitons [1]. TE, unlike other kinds of alopecia, is distinguished by diffuse hair loss without apparent scarring and often affects less than half of the hair on the scalp. TE, represents a prevalent form of non-scarring alopecia characterized by excessive shedding of hair, often triggered by physiological or psychological stressors.
Telogen effluvium appears 2 to 3 months after the underlying stressful situation or trigger. It may resolve on its own in some situations, but if the illness persists for more than 6 months, it is called chronic [2–3]. Individuals suffering from telogen effluvium frequently experience worry and excessive concern over their hair, which can have a substantial influence on their psychological well-being. While TE typically manifests as temporary hair loss, its impact on individuals' quality of life and self-esteem may be considerable [4–5].
Normal hair follicle activity is cyclical, including growth phase, involution phase, dormant phase, and release phase, which are termed as anagen, catagen, telogen and exogen respectively. The hair stays in the follicle for 4 to 6 weeks during telogen before starting the following anagen phase. A person's scalp has hundred thousand hairs on average, with the majority (86%) in the growth (anagen) phase. While, only 1% in the catagen phase, and the remainder (13%) in the telogen phase [6]. However, with telogen effluvium, the ratio switches to 70% growth (anagen) and 30% dormant (telogen) phases, resulting in up to 300 hairs lost every day. If the triggering cause is discovered, acute telogen effluvium can resolve on its own. It is critical to treat underlying scalp disorders such as psoriasis or seborrheic dermatitis, and quitting drugs suspected of causing the illness can be useful.
However, hair shedding that lasts for an extended period of time may suggest the presence of numerous causes, such as dietary deficits, thyroid disorders, systemic diseases, or infections [7–8]. This might complicate the search for triggers and necessitate many visits to address and manage these underlying problems. The basic method for treating chronic telogen effluvium is to reassure the patient and address any underlying reasons that have been found. However, PRP is an emerging therapy approach, and the effects of PRP on TE telogen conditions are yet to be fully identified.
PRP is a biological product derived from centrifuging a patient's blood, yielding a fraction of plasma with a greater concentration of platelets. The aforementioned includes several growth factors, chemokines, cytokines, and plasma proteins that may stimulate hair growth and neovascularization [9–11]. PRP has been widely utilized in several hair problems, including androgenetic alopecia; however, there is a dearth of well-designed trials testing its efficacy in individuals with persistent teloen effluvium [12]. As a result, it would be beneficial to undertake a study to evaluate the effectiveness and safety of PRP in chronic telogen effluvium.
This study aims to contribute to the evolving understanding of PRP's role in the management of TE. Additionally, the study seeks to assess the subjective experiences of patients undergoing PRP treatment, including pain perception and overall satisfaction. The primary objective of this study is to evaluate the effectiveness of PRP therapy in promoting hair regrowth as well as reducing hair shedding in patients with TE. Secondary objectives include assessing the safety profile of PRP treatment and exploring patient-reported outcomes such as improvement in hair density and quality of life measures.
Through rigorous evaluation and analysis, this research endeavors to provide important insights into the prospective benefits and limitations of PRP therapy as a therapeutic opportunity for TE, ultimately informing clinical practice and guiding future research directions in the field of hair disorders.
MATERIALS AND METHODS
Study Design and Setting
A single-blind, randomized clinical trial was conducted on patients diagnosed with telogen effluvium (TE). The study was carried out in the dermatology department at SLC Hospital in collaboration with IUL-H-PK.
Participants
The study targeted TE patients aged 20–40 years. A total of 60 patients were enrolled & randomly allocated into three groups (n = 20 per group).
Randomization and Allocation
Randomization was achieved using the envelope method. Patients were allocated to one of three treatment groups: Group A received combined therapy with Tressfix serum and PRP, Group B received PRP alone, and Group C received Tressfix serum alone.
Patient Selection Criteria
Inclusion criteria encompassed both male and female TE patients aged 20–40 years, excluding individuals with scalp-specific dermatological conditions such as psoriasis or seborrheic dermatitis, thyroid disorders, chronic medical illnesses, anemia (hemoglobin level <10 mg/dl), thrombocytopenia (platelet count <100,000/L), coagulopathies, or recent use of hair loss medications.
Intervention Strategy
PRP Treatment: Initially, venous blood (15 mL) was drawn from each patient using a 21-gauge butterfly needle to produce PRP via a double spin process. The blood was collected into five sterile tubes containing 3.8% sodium citrate as an anticoagulant. After centrifugation at 150 g for 10 minutes, the red blood cells were separated from the plasma, which contained the buffy coat of white blood cells and platelets. Subsequently, the plasma from each tube was moved to another tube and centrifuged for 10 minutes (room temperature) at 1500 - 2000 g. During the second centrifugation, the plasma was distributed into two portions: PRP & platelet-poor plasma (PPP). The PPP was aspirated first to prevent mixing with the PRP. Each tube's residual PRP was collected and activated by adding 0.1 mL of CaCl2 per 0.9 mL of PRP, resulting in an activated PRP concentration. This process yielded approximately 3 mL of PRP [13].
Injection: The PRP injection was administered intradermally using a 1-mL syringe and sterile 30-gauge needles. Following local anesthesia, 0.2 mL of PRP was injected into the subfollicular plane at 2 cm intervals on the scalp, including frontal, vertex and parietal sites. Proceeding to injection, the target scalp area was cleansed thoroughly using alcohol pads. Patients received one session every 02 weeks for a total of seven sessions over a 14-week period. Most patients reported significant pain improvement after the first or second session. Although some discomfort may occur, PRP injections are generally well-tolerated and not considered unpleasant [14].
Combination Therapy (Group A): Patients received PRP injections and applied Tressfix serum once daily for 14 weeks.
PRP Treatment (Group B): Patients underwent seven PRP sessions over 14 weeks.
Group A: Combination Therapy
- Participants in Group A showed to have a more pronounced impact on lowering microRNA expression related to Telogen effluvium compared to individual therapies.
Group B: PRP Alone Treatment
- Participants in Group B showed significant reductions in microRNA expression associated with Telogen effluvium.
Group C: Tressfix Serum Alone Treatment
- Participants in Group C did not exhibit significant changes in microRNA expression for five out of the nine microRNAs studied.
Tressfix Serum Treatment (Group C): Patients applied Tressfix serum daily for 14 weeks, containing Ginkgo biloba 4%, procapil 10%, panthenol 1%, biotin 2 mg, castor oil 2%, propylene glycol 5%, glycerin 5%, and wheat protein 5%.
Outcome Measures
Levels of Micro-Ribonucleic Acids
Levels of 15 different microRNAs were assessed, with nine miRNAs showing positive results. Quantitative RT-PCR analysis was performed on Bio-Rad CFX 96 Real-Time System.
MiRNA upregulation was detected by looking for upward-going sigmoid curves in the amplification plots, whereas downregulation was discovered by looking for straight lines.
Severity of Hair Loss
The severity of TE was evaluated using the Scalp Assessment of Hair Loss (SALT) score, from 0 to 100, higher scores representing higher severity of hair loss. Assessments were conducted at baseline, week 7, and week 14 [15].
The statistical analysis was carried out using appropriate methods, SEM and t-test was applied to compare treatment outcomes and evaluate the efficacy of the interventions.
RESULTS
Demographic Characteristics
The study enrolled participants with an average age of 38.65±6.56 years. The gender distribution included 25 (41.66%) male and 35 (58.33%) female participants.
Table 1: provides a detailed demographic description of the participants across the three treatment groups.
Table 1: Demographic Description of participants.
|
Variables |
Mean age in years ± SD |
Number of Males (%) |
Number of Females (%) |
|
Combine |
38.65±6.56years |
25 (41.66%) |
n=35 (58.33%). |
|
Group wise distribution |
|||
|
Group A (PRP + Tressfix Serum) |
38.99±4.25years |
9(36%) |
12(34.28%) |
|
Group B (PRP) |
35.55±1.1 years |
8(32%) |
11(31.42%) |
|
Group C (Tressfix Serum) |
35.78±2.1years |
8(32%) |
12(34.28%) |
The investigation revealed significant variations in microRNA (miRNA) expression levels among the treatment groups. In Group A (PRP + Tressfix Serum), miRNA expression was notably reduced compared to Groups B (PRP alone) and C (Tressfix Serum alone). Specifically, hsa-mir-223 and hsa-mir-212 exhibited considerably lower expression levels in Group A compared to the other groups, as depicted in Table 2.
Table 2: Levels of MicroRNA before and after intervention.
|
Variables |
Pre mean ± SD |
Post mean ± SD |
MD ± sd |
t-stats |
p-value |
|
|
Group A |
hsa-mir- 223 |
153.65±3.58 |
113.53±2.95 |
40.12±5.68 |
4.56 |
<0.001 |
|
hsa-mir- 212 |
95.68±2.56 |
53.5±7.56 |
42.18±6.84 |
.21 |
<0.001 |
|
|
hsa-mir-21 |
135.48±3.65 |
109.32±5.55 |
26.1±4.48 |
5.65 |
<0.001 |
|
|
hsa-mir-421 |
136.58±3.53 |
109.88±2.25 |
26.7±4.22 |
8.92 |
<0.001 |
|
|
hsa-mir-29b-1 |
95.68±4.55 |
63.58±5.12 |
32.01±4.43 |
9.36 |
<0.001 |
|
|
hsa-mir-941 |
82.55±2.28 |
52.13±1.56 |
30.42±7.01 |
7.57 |
<0.001 |
|
|
hsa-miR-155 |
117.58±7.59 |
99.89±5.48 |
17.69±5.41 |
6.89 |
<0.001 |
|
|
hsa-miR-98 |
115.25±11.25 |
102.56±3.58 |
12.64±5.11 |
8.58 |
<0.001 |
|
|
hsa-miR-10a |
96.48±5.82 |
75.88±6.25 |
20.6±6.3 |
11.5 |
<0.001 |
|
|
Group B |
hsa-mir- 223 |
161.59±3.47 |
140.21±5.56 |
21.38±6.55 |
5.22 |
<0.001 |
|
hsa-mir- 212 |
93.12±7.15 |
75.58±8.71 |
17.54±4.58 |
11.47 |
<0.001 |
|
|
hsa-mir-21 |
130.14±2.58 |
125.56±6.58 |
4.58±1.11 |
6.25 |
<0.001 |
|
|
hsa-mir-421 |
130.78±4.55 |
128.56±3.34 |
2.22±1.2 |
3.66 |
0.05 |
|
|
hsa-mir-29b-1 |
85.56±3.55 |
69.11±2.52 |
16.45±4.21 |
10.58 |
<0.001 |
|
|
hsa-mir-941 |
77.45±2.33 |
63.58±3.58 |
13.87±2.21 |
9.58 |
<0.001 |
|
|
hsa-miR-155 |
120.55±7.59 |
109.58±6.14 |
10.97±3.35 |
2.5 |
<0.001 |
|
|
hsa-miR-98 |
113.47±10.13 |
105.56±7.91 |
7.91±4.41 |
1.3 |
<0.001 |
|
|
hsa-miR-10a |
95.12±5.82 |
83.25±3.30 |
11.87±2.24 |
11.9 |
<0.001 |
|
|
Group C |
hsa-mir- 223 |
165.25±6.59 |
163.22±2.37 |
2.03±1.001 |
1.11 |
0.05 |
|
hsa-mir- 212 |
95.54±5.13 |
87.12±6.9 |
8.33±4.37 |
2.38 |
<0.01 |
|
|
hsa-mir-21 |
131.44±4.45 |
129.11±6.35 |
2.33±1.20 |
3.1 |
0.56 |
|
|
hsa-mir-421 |
129.65±3.22 |
128.45±6.32 |
1.2±0.58 |
1.52 |
0.06 |
|
|
hsa-mir-29b-1 |
88.96±2.09 |
85.15±5.42 |
3.81±1.01 |
1.54 |
0.055 |
|
|
hsa-mir-941 |
81.25±2.36 |
73.56±5.25 |
7.69±2.11 |
3.98 |
<0.001 |
|
|
hsa-miR-155 |
125.65±325 |
123.11±5.5 |
2.54±2.01 |
0.25 |
0.055 |
|
|
hsa-miR-98 |
115.65±2.58 |
114.98±1.98 |
0.7±0.14 |
2.65 |
0.8 |
|
|
hsa-miR-10a |
98.78±3.56 |
95.65±2.85 |
3.13±1.55 |
3.98 |
0.05 |
|
Group A demonstrated a mean difference (MD) ± standard deviation (SD) of 40.12±5.68 for hsa-mir-223 and 42.18±6.84 for hsa-mir-212 compared to Group B, indicating a significant impact of the combined therapy on miRNA expression associated with telogen effluvium. Additionally, hsa-mir-21, hsa-mir-421, hsa-mir-29b-1, hsa-mir-941, hsa-miR-155, hsa-miR-98, and hsa-miR-10a also exhibited substantial reductions in expression levels in Group A.
In Group B, while miRNA expression was lower compared to Group C, it was higher than Group A for hsa-mir-223 and hsa-mir-212. Notably, hsa-mir-21, hsa-mir-29b-1, hsa-mir-941, hsa-miR-155, hsa-miR-98, and hsa-miR-10a showed significant reductions in expression levels post-treatment.
Group C demonstrated the highest miRNA expression levels among the three groups, with minimal reductions observed post-treatment. However, the expressions of hsa-mir-223 and hsa-mir-212 were significantly lower in Group C compared to baseline.
Scalp Assessment of Hair Loss (SALT) Score
The SALT score analysis revealed significant improvements in all three-treatment groups from baseline to week 14. Group A, exhibited the most substantial reduction in the SALT score, indicating a greater improvement in scalp health compared to Groups B and C. Table 3 summarizes the changes in the SALT score at baseline, week 7, and week 14 for each treatment group.
Table 3: Analyses of the effects of treatment strategies on SALT score.
|
Variables |
Baseline ± SD |
At week 7 ± SD |
After intervention week 14 ± SD |
Level of significance |
|
Group A |
80.13±4.28 |
43.58±2.57 |
25.65±4.58 |
p<0.001 |
|
Group B |
85.58±2.65 |
60.39±4.58 |
32.47±3.25 |
|
|
Group C |
85.24±2.11 |
68.14±5.22 |
45.58±4.21 |
Overall, the combination therapy of PRP and Tressfix Serum (Group A) demonstrated superior efficacy in reducing miRNA expression associated with hair loss and improving the SALT score compared to monotherapy or serum alone. These findings underscore the potential synergistic effects of combined treatments in managing telogen effluvium and enhancing scalp health.
DISCUSSION
The observed downregulation of specific miRNAs, such as hsa-mir-223 and hsa-mir-212, following combined PRP and Tressfix Serum therapy aligns with previous research implicating these miRNAs in hair follicle cycling and regeneration [16,17]. Hsa-mir-223 has been associated with the suppression of hair growth by targeting key genes involved in hair follicle development as well as cycling, while, hsa-mir-212 has been implicated in the regulation of hair follicle stem cell proliferation and differentiation [16,17]. The significant reductions in miRNA expression levels post-treatment suggest a restoration of hair follicle homeostasis and a potential shift from the telogen to the anagen phase, promoting hair growth and thickness.
Moreover, synergistic effects of PRP and Tressfix Serum may extend beyond miRNA modulation to include enhanced angiogenesis, tissue regeneration, and growth factor signaling within the hair follicle microenvironment [18,19]. PRP, enriched with various growth factors and cytokines, has been shown to stimulate hair follicle stem cells, promote neovascularization, and modulate inflammation, contributing to hair regeneration and maintenance [18,19]. Tressfix Serum, with its proprietary blend of botanical extracts and peptides, may complement PRP therapy by providing additional nourishment and support to the hair follicles, thereby optimizing treatment outcomes.
The significant improvements in the SALT score across all treatment groups underscore the clinical efficacy of the interventions in promoting scalp health and mitigating hair loss symptoms. The SALT score serves as a valuable tool for objectively assessing hair loss severity and treatment response, facilitating personalized treatment strategies and monitoring of disease progression [20,21]. The observed correlation between miRNA expression levels and SALT scores reflects the prospective usefulness of miRNAs as biomarkers for monitoring treatment response and predicting long-term outcomes in individuals with hair loss disorders.
Additional Perspectives
Further research is warranted to elucidate the underlying molecular mechanisms driving the observed changes in miRNA expression patterns and treatment outcomes. Transcriptomic and proteomic analyses may provide valuable insights into the downstream signaling pathways and molecular targets modulated by PRP and Tressfix Serum therapy, offering new avenues for therapeutic intervention and drug development [22]. It is needed to have studies with longer duration, larger sample sizes. Moreover, diverse patient populations are required to validate the reproducibility and generalizability of the findings across different demographic and clinical contexts.
Moreover, the integration of emerging technologies such as exosome therapy, microneedling, and low-level laser therapy (LLLT) may offer synergistic benefits and enhance the efficacy of existing treatment modalities for hair loss [23,24]. Exosomes, as potent carriers of bioactive molecules and regulatory RNAs, hold promise for promoting tissue regeneration, modulating inflammation, and restoring hair follicle function. Microneedling, by inducing controlled microtrauma and releasing growth factors, may enhance the penetration and efficacy of topical treatments such as Tressfix Serum, facilitating hair follicle regeneration and neovascularization [23]. LLLT, through its photobiomodulatory effects on cellular metabolism and gene expression, may stimulate hair follicle stem cells and promote hair growth, particularly when combined with PRP therapy [24].
STRENGTHS
- Comprehensive assessment of miRNA expression patterns and treatment outcomes using a well-defined study protocol.
- Inclusion of the SALT score as an objective measure of treatment response, providing clinically relevant insights into scalp health improvement.
- Rigorous statistical analysis and subgroup comparisons to elucidate treatment effects and identify potential synergies between therapeutic modalities.
LIMITATIONS
- Relatively small sample size and single-center study design may limit the generalizability of the findings.
- Lack of long-term follow-up data to assess the durability and sustainability of treatment effects over time.
- Potential confounding factors such as concomitant medications and lifestyle factors were not systematically accounted for in the analysis.
Despite these limitations, the study contributes valuable evidence to the field of hair loss research and underscores the need for further investigation into optimal treatment strategies and personalized approaches to hair loss management.
CONCLUSION
In conclusion, the findings of the study show that combining platelet-rich plasma (PRP) with Tressfix serum results in significant decreases in microRNA expression associated with telogen effluvium. The results show that Group A (PRP and Tressfix serum combined) and Group B (PRP alone) had considerably lower levels of expression for all microRNAs than Group C (Tressfix serum alone). These data imply that combining PRP with Tressfix serum therapy may have a more dramatic effect on microRNA expression and may provide greater therapeutic advantages in the management of telogen effluvium as compared to separate therapies. To confirm and expand on these findings, further research on larger sample numbers and follow-up times is required.
Conflict of Interest Disclosure
The Authors have no conflict of interest.
Financial Disclosure
The authors declared that this study received no financial support.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Consent
This work has not been published previously, is not under consideration for publication elsewhere, and has not been accepted for publication elsewhere.
Patient Consent
Written informed consent was obtained from all participants.
Acknowledgments
In compliance with the ICMJE uniform disclosure form the authors acknowledge all investigators, staff at the participating centers and all patients for their commitment to the study. UR, AF participated in the study design, data collection, drafting and critical review. SQ and AF, performed data collection, analysis and wrote the description and Discussion of the results. UR, AF, SQ, NK participated in the finalization of the article. All authors read and approved the final manuscript. All authors read and approved the final manuscript.
Ethical Approval and Consent to Participate
The study was approved by institutional ethics committees Board of dermatology at SL-Care Hospital, Hyderabad in collaboration with IUL University Pakistan. All patients signed a consent form. The study was a prospective, non-interventional study in compliance with the Declaration of Helsinki.
REFERENCES
- Burroway B, Griggs J, Martinez-Velasco MA. (2020). Tosti Telogen Effluvium. Hair and Scalp Treatments: A Practical Guide. 2020:125–138.
- Mohammad AP, Baba AT, Ghassemi MO. (2020). Comparison between serum levels of vitamin D and zinc in women with diffuse non-scarring hair loss (telogen effluvium) and healthy women. Pakistan J Med Hlth Sci. 14:1400–1404.
- Nagar N, Garg P, Poswal RK, Kumar A, Singhal K. (2023). Telogen effluvium hair loss and its homoeopathic approach. 6(2).
- Asghar F, Shamim N, Farooque U, Sheikh H, Aqeel R. (2020). Telogen effluvium: a review of the literature. 12(5):e8320.
- Mellaratna WP, Kholilullah VZ. (2023). Telogen Effluvium. Galenical. 2(3):76-88.
- Alessandrini A, Bruni F, Piraccini BM, Starace M. (2021). Common causes of hair loss - clinical manifestations, trichoscopy and therapy. J Eur Acad Dermatol Venereol. 35(3):629-640.
- Domínguez-Santás M, Haya-Martínez L, Fernández-Nieto D, Jiménez-Cauhé J, Suárez-Valle A, Díaz-Guimaraens B. (2020). Acute telogen effluvium associated with SARS-CoV-2. Aust J Gen Pract. 49:32.
- Chien Yin GO, Siong-See JL, Wang ECE. (2021). Telogen Effluvium—a review of the science and current obstacles. J DermatolSci. 101(3):156-163.
- Rebora A. (2019). Telogen effluvium: a comprehensive review. Clin Cosmet Investig Dermatol. 583-590.
- Coleman E. Types and treatment of hair loss in men and women. Plastic and Aesthetics 2020; 40(4):222-235.
- Mysore V, Parthasaradhi A, Kharkar RD, Ghoshal AK, Ganjoo A, Ravichandran G, et al. (2019). Expert consensus on the management of telogen effluvium in India. Int J Trich. 11(3):107.
- Deng T, Ngo T, Zhu, TH, Halverstam C. (2021). Telogen effluvium, Beau lines, and acral peeling are associated with COVID-19 infection. JAAD Case Rep. 13:138–140.
- Zhang W, Guo Y, Kuss M, Shi W, Aldrich AL, Untrauer J, et al. (2019). Platelet-rich plasma for the treatment of tissue infection: preparation and clinical Tissue Engineering Part B: Reviews. 25(3):225-236.
- Filardo G, Previtali D, Napoli F, Candrian C, Zaffagnini S, Grassi A. (2021). PRP injections for the treatment of knee osteoarthritis: a meta-analysis of randomized controlled trials. 13(1_suppl):364S-375S.
- Wyrwich KW, Kitchen H, Knight S, Aldhouse NV, Macey J, Nunes FP, et al. (2020). The Alopecia Areata Investigator Global Assessment Scale is a measure for evaluating clinically meaningful success in clinical trials. BritJ Dermat. 183(4):702–709.
- Mokabber H, Vatankhah MA, Najafzadeh N. (2022). The regulatory role of microRNAs in the development, cyclic changes, and cell differentiation of the hair follicle. Process Biochemistry. 114:36-41.
- Zhu N, Huang K, Liu Y, Zhang H, Lin E, Zeng Y, et al. (2018). miR-195-5p Regulates Hair Follicle Inductivity of Dermal Papilla Cells by Suppressing Wnt/β-Catenin Activation. Biomed Res Int. 2018:4924356.
- Wang W, Wang H, Long Y, Li Z, Li J. (2023). Controlling Hair Loss by Regulating Apoptosis in Hair Follicles: A Comprehensive Overview. Biomolecules. 14(1):20.
- Juhasz MLW, Lo Sicco K, Shapiro J. (2020). The Utility of Platelet-Rich Plasma for the Treatment of Alopecia. J Drugs Dermatol. 19(7):736-741.
- Cruciani M, Masiello F, Pati I, Marano G, Pupella S, De Angelis V. (2023). Platelet-rich plasma for the treatment of alopecia: a systematic review and meta-analysis. Blood Transfus. 21(1):24-36.
- Hegde P, Relhan V, Sahoo B, Garg VK. (2020). A randomized, placebo and active controlled, split scalp study to evaluate the efficacy of platelet-rich plasma in patchy alopecia areata of the scalp. Dermatol Ther. 33(6):e14388.
- Paichitrojjana A, Paichitrojjana A. (2022). Platelet Rich Plasma and Its Use in Hair Regrowth: A Review. Drug Des Devel Ther. 16:635-645.
- Pei D, Zeng L, Huang X, Wang B, Liu L, Zhang G. (2024). Efficacy and safety of combined microneedling therapy for androgenic alopecia: A systematic review and meta-analysis of randomized clinical trials. J Cosmet Dermatol. 18.
- Liu D, Xu Q, Meng X, Liu X, Liu J. (2024). Status of research on the development and regeneration of hair follicles. Int J Med Sci. 21(1):80-94.